
Simultaneous Determination of Antibodies to Pertussis Toxin and Adenylate Cyclase Toxin Improves Serological Diagnosis of Pertussis

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Serum Samples and Reference Assays
2.2. Lateral Flow Test Strips and Multiplex Assay
2.3. Statistics
3. Results
3.1. Specificity and Overall Assay Performance
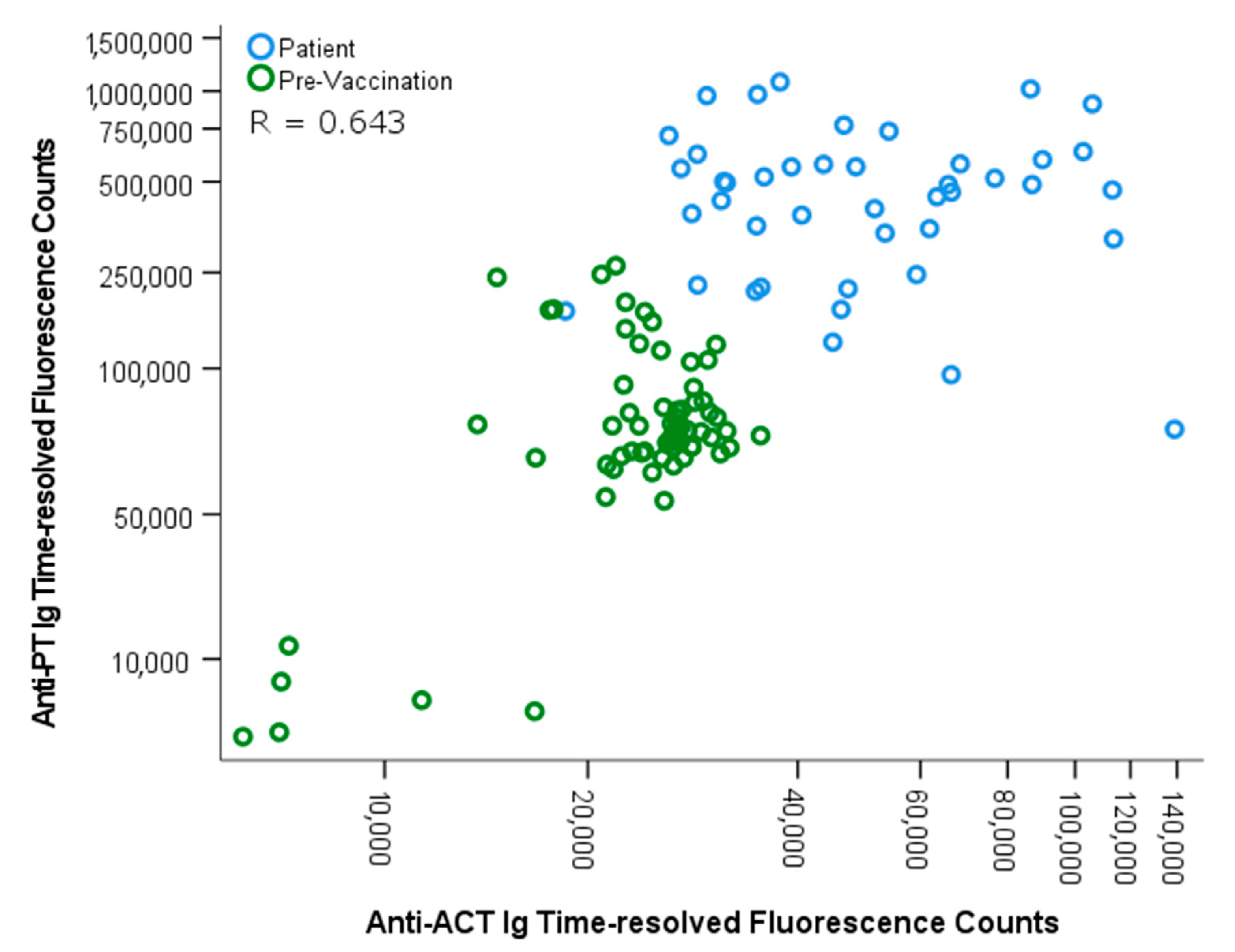
3.2. Differentiation between Vaccination and Infection
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pebody, R.G.; Gay, N.J.; Giammanco, A.; Baron, S.; Schellekens, J.; Tischer, A.; Olander, N.J.; Andrews, N.J.; Edmunds, W.J.; Lecoeur, H.; et al. The seroepidemiology of Bordetella pertussis infection in Western Europe. Epidemiol. Infect. 2005, 133, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Barkoff, A.M.; Grondahl-Yli-Hannuksela, K.; He, Q. Seroprevalence studies of pertussis: What have we learned from different immunized populations. Pathog Dis. 2015, 73. [Google Scholar] [CrossRef] [Green Version]
- Dalby, T.; Petersen, J.W.; Harboe, Z.B.; Krogfelt, K.A. Antibody responses to pertussis toxin display different kinetics after clinical Bordetella pertussis infection than after vaccination with an acellular pertussis vaccine. J. Med. Microbiol. 2010, 59, 1029–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, L.; Hallander, H.O.; Olin, P.; Reizenstein, E.; Storsaeter, J. A controlled trial of a two-component acellular, a five-component acellular, and a whole-cell pertussis vaccine. N. Engl. J. Med. 1996, 334, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Arciniega, J.L.; Hewlett, E.L.; Johnson, F.D.; Deforest, A.; Wassilak, S.G.; Onorato, I.M.; Manclark, C.R.; Burns, D.L. Human serologic response to envelope-associated proteins and adenylate cyclase toxin of Bordetella pertussis. J. Infect. Dis. 1991, 163, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Confer, D.L.; Eaton, J.W. Phagocyte impotence caused by an invasive bacterial adenylate cyclase. Science 1982, 217, 948–950. [Google Scholar] [CrossRef] [PubMed]
- Guiso, N.; Grimprel, E.; Anjak, I.; Begue, P. Western blot analysis of antibody responses of young infants to pertussis infection. Eur. J. Clin. Microbiol. Infect. Dis. 1993, 12, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Sebo, P.; Osicka, R.; Masin, J. Adenylate cyclase toxin-hemolysin relevance for pertussis vaccines. Expert Rev. Vaccines 2014, 13, 1215–1227. [Google Scholar] [CrossRef]
- Subissi, L.; Rodeghiero, C.; Martini, H.; Litzroth, A.; Huygen, K.; Leroux-Roels, G.; Pierard, D.; Desombere, I. Assessment of IgA anti-PT and IgG anti-ACT reflex testing to improve Bordetella pertussis serodiagnosis in recently vaccinated subjects. Clin. Microbiol. Infect. 2019, 26, 645-e1. [Google Scholar] [CrossRef]
- Watanabe, M.; Connelly, B.; Weiss, A.A. Characterization of serological responses to pertussis. Clin. Vaccine Immunol. 2006, 13, 341–348. [Google Scholar] [CrossRef] [Green Version]
- Guiso, N.; Berbers, G.; Fry, N.K.; He, Q.; Riffelmann, M.; von Konig, C.W.; EU Pertstrain Group. What to do and what not to do in serological diagnosis of pertussis: Recommendations from EU reference laboratories. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 307–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knuutila, A.; Rautanen, C.; Mertsola, J.; He, Q. Multiplex Point-of-Care Tests for the Determination of Antibodies after Acellular Pertussis Vaccination. Diagnostics 2020, 10, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran Minh, N.N.; He, Q.; Ramalho, A.; Kaufhold, A.; Viljanen, M.K.; Arvilommi, H.; Mertsola, J. Acellular vaccines containing reduced quantities of pertussis antigens as a booster in adolescents. Pediatrics 1999, 104, e70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Q.; Mertsola, J.; Himanen, J.P.; Ruuskanen, O.; Viljanen, M.K. Evaluation of pooled and individual components of Bordetella pertussis as antigens in an enzyme immunoassay for diagnosis of pertussis. Eur. J. Clin. Microbiol. Infect. Dis. 1993, 12, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Barkoff, A.M.; Grondahl-Yli-Hannuksela, K.; Vuononvirta, J.; Mertsola, J.; Kallonen, T.; He, Q. Differences in avidity of IgG antibodies to pertussis toxin after acellular pertussis booster vaccination and natural infection. Vaccine 2012, 30, 6897–6902. [Google Scholar] [CrossRef] [PubMed]
- Reizenstein, E.; Hallander, H.O.; Blackwelder, W.C.; Kuhn, I.; Ljungman, M.; Mollby, R. Comparison of five calculation modes for antibody ELISA procedures using pertussis serology as a model. J. Immunol. Methods 1995, 183, 279–290. [Google Scholar] [CrossRef]
- Osicka, R.; Osickova, A.; Basar, T.; Guermonprez, P.; Rojas, M.; Leclerc, C.; Sebo, P. Delivery of CD8(+) T-cell epitopes into major histocompatibility complex class I antigen presentation pathway by Bordetella pertussis adenylate cyclase: Delineation of cell invasive structures and permissive insertion sites. Infect. Immun. 2000, 68, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Sadilkova, L.; Osicka, R.; Sulc, M.; Linhartova, I.; Novak, P.; Sebo, P. Single-step affinity purification of recombinant proteins using a self-excising module from Neisseria meningitidis FrpC. Protein Sci. 2008, 17, 1834–1843. [Google Scholar] [CrossRef] [Green Version]
- Stanek, O.; Masin, J.; Osicka, R.; Jurnecka, D.; Osickova, A.; Sebo, P. Rapid Purification of Endotoxin-Free RTX Toxins. Toxins 2019, 11, 336. [Google Scholar] [CrossRef] [Green Version]
- Salminen, T.; Knuutila, A.; Barkoff, A.M.; Mertsola, J.; He, Q. A rapid lateral flow immunoassay for serological diagnosis of pertussis. Vaccine 2018, 36, 1429–1434. [Google Scholar] [CrossRef]
- Giammanco, A.; Taormina, S.; Chiarini, A.; Dardanoni, G.; Stefanelli, P.; Salmaso, S.; Mastrantonio, P. Analogous IgG subclass response to pertussis toxin in vaccinated children, healthy or affected by whooping cough. Vaccine 2003, 21, 1924–1931. [Google Scholar] [CrossRef]
- Hendrikx, L.H.; Schure, R.M.; Ozturk, K.; de Rond, L.G.; de Greeff, S.C.; Sanders, E.A.; Berbers, G.; Buisman, A.M. Different IgG-subclass distributions after whole-cell and acellular pertussis infant primary vaccinations in healthy and pertussis infected children. Vaccine 2011, 29, 6874–6880. [Google Scholar] [CrossRef] [PubMed]
- Nagel, J.; de Graaf, S.; Schijf-Evers, D. Improved serodiagnosis of whooping cough caused by Bordetella pertussis by determination of IgG anti-LPF antibody levels. Dev. Biol. Stand. 1985, 61, 325–330. [Google Scholar] [PubMed]
- Poynten, M.; Hanlon, M.; Irwig, L.; Gilbert, G.L. Serological diagnosis of pertussis: Evaluation of IgA against whole cell and specific Bordetella pertussis antigens as markers of recent infection. Epidemiol. Infect. 2002, 128, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.G.; Ashworth, L.A.; Miller, E.; Lambert, H.P. Serum IgG, IgA, and IgM responses to pertussis toxin, filamentous hemagglutinin, and agglutinogens 2 and 3 after infection with Bordetella pertussis and immunization with whole-cell pertussis vaccine. J. Infect. Dis. 1989, 160, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Grimprel, E.; Begue, P.; Anjak, I.; Njamkepo, E.; Francois, P.; Guiso, N. Long-term human serum antibody responses after immunization with whole-cell pertussis vaccine in France. Clin. Diagn. Lab. Immunol. 1996, 3, 93–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherry, J.D.; Xing, D.X.; Newland, P.; Patel, K.; Heininger, U.; Corbel, M.J. Determination of serum antibody to Bordetella pertussis adenylate cyclase toxin in vaccinated and unvaccinated children and in children and adults with pertussis. Clin. Infect. Dis. 2004, 38, 502–507. [Google Scholar] [CrossRef] [Green Version]
- Linhartova, I.; Bumba, L.; Masin, J.; Basler, M.; Osicka, R.; Kamanova, J.; Prochazkova, K.; Adkins, I.; Hejnova-Holubova, J.; Sadilkova, L.; et al. RTX proteins: A highly diverse family secreted by a common mechanism. FEMS Microbiol. Rev. 2010, 34, 1076–1112. [Google Scholar] [CrossRef] [Green Version]
- Betsou, F.; Sismeiro, O.; Danchin, A.; Guiso, N. Cloning and sequence of the Bordetella bronchiseptica adenylate cyclase-hemolysin-encoding gene: Comparison with the Bordetella pertussis gene. Gene 1995, 162, 165–166. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N | Age (Range) | Median ELISA Anti-PT IgG (IU/mL) (Range) | |
|---|---|---|---|
| Patient | 46 | 3–70 | 283 (50–1041) |
| Healthy | 102 | 20–39 | 0–1 |
| Pre-vaccination | 67 | 11–13 | 9 (3–279) |
| Post-vaccination | 67 | 11–13 | 109 (15–755) |
| Diagnostic Antigen(s) | Patients, Total n = 46 (Sensitivity %) | Pre-Vaccination, Total n = 67 (Specificity %) | Post-Vaccination, Total n = 67 (Specificity %) |
|---|---|---|---|
| PT 1 | 36 (78.2) | 1 (98.5) | 37 (44.8) |
| ACT 2 | 31 (69.6) | 0 (100) | 0 (100) |
| PT and ACT 3 | 42 (91.3) | 1 (98.5) | 37 (44.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knuutila, A.; Barkoff, A.-M.; Mertsola, J.; Osicka, R.; Sebo, P.; He, Q. Simultaneous Determination of Antibodies to Pertussis Toxin and Adenylate Cyclase Toxin Improves Serological Diagnosis of Pertussis. Diagnostics 2021, 11, 180. https://doi.org/10.3390/diagnostics11020180
Knuutila A, Barkoff A-M, Mertsola J, Osicka R, Sebo P, He Q. Simultaneous Determination of Antibodies to Pertussis Toxin and Adenylate Cyclase Toxin Improves Serological Diagnosis of Pertussis. Diagnostics. 2021; 11(2):180. https://doi.org/10.3390/diagnostics11020180
Chicago/Turabian StyleKnuutila, Aapo, Alex-Mikael Barkoff, Jussi Mertsola, Radim Osicka, Peter Sebo, and Qiushui He. 2021. "Simultaneous Determination of Antibodies to Pertussis Toxin and Adenylate Cyclase Toxin Improves Serological Diagnosis of Pertussis" Diagnostics 11, no. 2: 180. https://doi.org/10.3390/diagnostics11020180