High-Performance Liquid Chromatography as a Novel Method for the Determination of α-Defensins in Synovial Fluid for Diagnosis of Orthopedic Infections


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
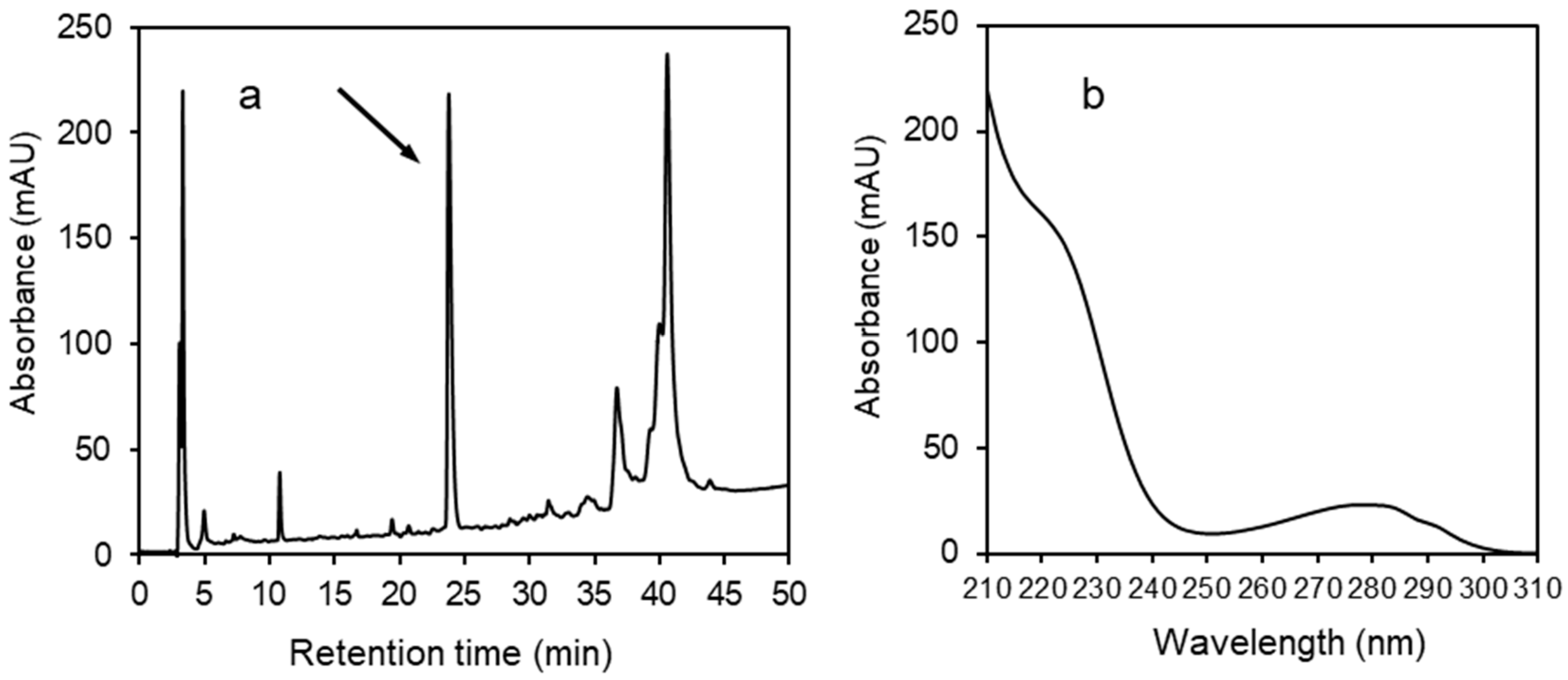
2.2. HPLC Analysis
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Parvizi, J. Diagnosing periprosthetic joint infection. Has the era of the biomarker arrived? Clin. Orthop. Relat. Res. 2014, 472, 3254–3262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Springer, B.D. The diagnosis of periprosthetic joint infection. J. Arthroplast. 2015, 30, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.K.; Huang, B.; Bae, E.K.; Park, E.J.; Hwang, J.W.; Lee, J.; Koh, E.M.; Cha, H.S. The role of α-defensin-1 and related signal transduction mechanisms in the production of IL-6, IL-8 and MMPs in rheumatoid fibroblast-like synoviocytes. Rheumatology 2013, 52, 1368–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Parvizi, J. Combined measurement of synovial fluid α-defensin and C-reactive protein levels: Highly accurate for diagnosing periprosthetic joint infection. J. Bone Jt. Surg. Am. 2014, 96, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Booth, R.E., Jr.; Parvizi, J. The alpha-defensin test for periprosthetic joint infection outperforms the leukocyte esterase test strip. Clin. Orthop. Relat. Res. 2015, 473, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frangiamore, S.J.; Gajewski, N.D.; Saleh, A.; Farias-Kovac, M.; Barsoum, W.K.; Higuera, C.A. α-Defensin accuracy to diagnose periprosthetic joint infection—Best available test? J. Arthroplast. 2016, 31, 456–460. [Google Scholar] [CrossRef]
- Ganz, T. Defensins: Antimicrobial peptides of innate immunity. Nat. Rev. Immunol. 2003, 3, 710–720. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, R.I.; Lu, W. α-Defensins in human innate immunity. Immunol. Rev. 2012, 245, 84–112. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Ericksen, B.; Tucker, K.; Lubkowski, J.; Lu, W. Synthesis and characterization of human α-defensins 4-6. J. Pept. Res. 2004, 64, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Pupaibool, J.; Fulnecky, E.J.; Swords, R.L., Jr.; Sistrunk, W.W.; Haddow, A.D. Alpha-defensin-novel synovial fluid biomarker for the diagnosis of periprosthetic joint infection. Int. Orthop. 2016, 40, 2447–2452. [Google Scholar] [CrossRef] [PubMed]
- Berger, P.; Van Cauter, M.; Driesen, R.; Neyt, J.; Cornu, O.; Bellemans, J. Diagnosis of prosthetic joint infection with alpha-defensin using a lateral flow device: A multicentre study. Bone Jt. J. 2017, 99, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, T.; Lausmann, C.; Citak, M.; Bonanzinga, T.; Frommelt, L.; Zahar, A. The accuracy of the alpha defensin lateral flow device for diagnosis of periprosthetic joint infection: Comparison with a gold standard. J. Bone Jt. Surg. Am. 2018, 100, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Bonanzinga, T.; Zahar, A.; Dütsch, M.; Lausmann, C.; Kendoff, D.; Gehrke, T. How reliable is the alpha-defensin immunoassay test for diagnosing periprosthetic joint infection? A prospective study. Clin. Orthop. Relat. Res. 2017, 475, 408–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigmund, I.K.; Holinka, J.; Gamper, J.; Staats, K.; Böhler, C.; Kubista, B.; Windhager, R. Qualitative α-defensin test (Synovasure) for the diagnosis of periprosthetic infection in revision total joint arthroplasty. Bone Jt. J. 2017, 99, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Sigmund, I.K.; Yermak, K.; Perka, C.; Trampuz, A. Is the enzyme-linked immunosorbent assay more accurate than the lateral flow alpha defensin test for diagnosing periprosthetic joint infection? Clin. Orthop. Relat. Res. 2018, 476, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, S.; Al-Mansoori, A.A.; Chand, M.R.; Villa, J.M.; Suarez, J.C.; Patel, P.D. What is the optimal criteria to use for detecting periprosthetic joint infections before total joint arthroplasty? J. Arthroplast. 2018, 33, S201–S204. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T. Definition of periprosthetic joint infection. J. Arthroplast. 2014, 29, 1331. [Google Scholar] [CrossRef] [Green Version]
- Zmistowski, B.; Della Valle, C.; Bauer, T.W.; Malizos, K.N.; Alavi, A.; Bedair, H.; Booth, R.E.; Choong, P.; Deirmengian, C.; Ehrlich, G.D.; et al. Diagnosis of Periprosthetic Joint Infection. J. Orthop. Res. 2014, 32, S98–S107. [Google Scholar] [CrossRef]
- de Saint Vincent, B.; Migaud, H.; Seneeville, E.; Loiez, C.; Pasquier, G.; Girard, J.; Putman, S. Diagnostic accuracy of the alpha defensin lateral flow device (Synovasure) for periprosthetic infections in microbiologically complex situations: A study of 42 cases in a French referral centre. Orthop. Traumatol. Surg. Res. 2018, 148, 427–431. [Google Scholar] [CrossRef]
- Kasparek, M.F.; Kasparek, M.; Boettner, F.; Faschingbauer, M.; Hahne, J.; Dominkus, M. Intraoperative diagnosis of periprosthetic joint infection using a novel alpha-defensin lateral flow assay. J. Arthroplast. 2016, 31, 2871–2874. [Google Scholar] [CrossRef]
- Scholten, R.; Visser, J.; van Susante, J.L.C.; van Loon, C.J.M. Low sensitivity of α-defensin (Synovasure) test for intraoperative exclusion of prosthetic joint infection. Acta Orthop. 2018, 89, 357–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partridge, D.G.; Gordon, A.; Townsend, R. False-positive synovial fluid alpha-defensin test in patient with acute gout affecting a prosthetic knee. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 549–551. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, F.; Pufe, T.; Conradi, L.; Varoga, D.; Tsokos, M.; Papendieck, J.; Petersen, W. Antimicrobial peptides are expressed and produced in healthy and inflamed human synovial membranes. J. Pathol. 2002, 198, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.S.; Hirschmann, M.T.; Becker, R.; Shaker, A.; Ateschrang, A.; Keel, M.J.B.; Albers, C.E.; Buetikofer, L.; Maqungo, S.; Stöckle, U.; et al. A meta-analysis of synovial biomarkers in periprosthetic joint infection: Synovasure™ is less effective than the ELISA-based alpha-defensin test. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3039–3047. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient | Cultivation | PCR | AD by HPLC | Diagnosis |
|---|---|---|---|---|
| 1 | neg. | pos. | pos. | IA |
| 2 | neg. | pos. | pos. | IA |
| 3 | neg. | pos. | pos. | IA |
| 4 | neg. | neg. | pos. | IA |
| 5 | neg. | pos. | pos. | IA |
| 6 | neg. | pos. | pos. | IA |
| 7 | pos. | pos. | pos. | PJI |
| 8 | neg. | pos. | pos. | PJI |
| 9 | pos. | pos. | pos. | PJI |
| 10 | neg. | pos. | pos. | PJI |
| 11 | neg. | pos. | pos. | PJI |
| 12 | neg. | pos. | pos. | PJI |
| 13 | neg. | neg. | pos. | PJI |
| 14 | neg. | neg. | neg. | TEP * |
| 15 | neg. | pos. | neg. | TEP * |
| 16 | neg. | neg. | neg. | TEP * |
| 17 | neg. | neg. | neg. | TEP * |
| 18 | neg. | neg. | neg. | TEP * |
| 19 | neg. | neg. | pos. | REA * |
| 20 | neg. | neg. | neg. | REA * |
| 21 | neg. | neg. | neg. | RHA * |
| 22 | neg. | neg. | neg. | AR * |
| 23 | neg. | neg. | neg. | AR * |
| 24 | neg. | neg. | neg. | AR * |
| Viewpoint | Synovasure® PJI Test (Lateral Flow Device) | ELISA | HPLC |
|---|---|---|---|
| α-defensins | Sum of HNP1–3 | HNP1, HNP3, or sum of HNP1–3 | Sum of HNP1–3 |
| Type of examination | Diagnostic device | Laboratory exam using diagnostic kit | Laboratory exam using instrument |
| Test output | Presence/absence of PJI | Exact concentration of single α-defensin | Exact concentration of the sum of α-defensins |
| Time to result | Within 10 min | Within hours | Within 1 h |
| Cost | Expensive | Less expensive | Low cost |
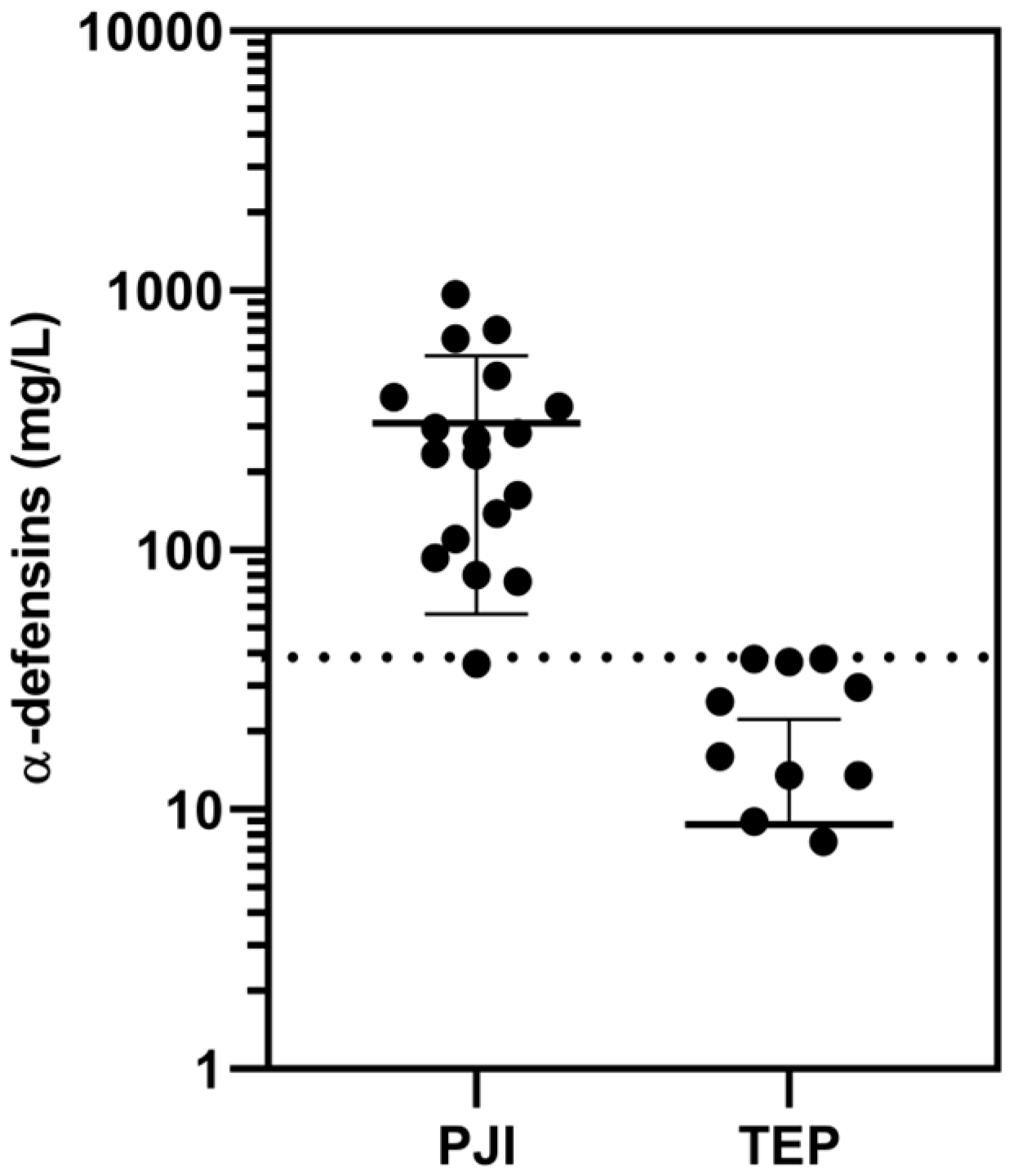
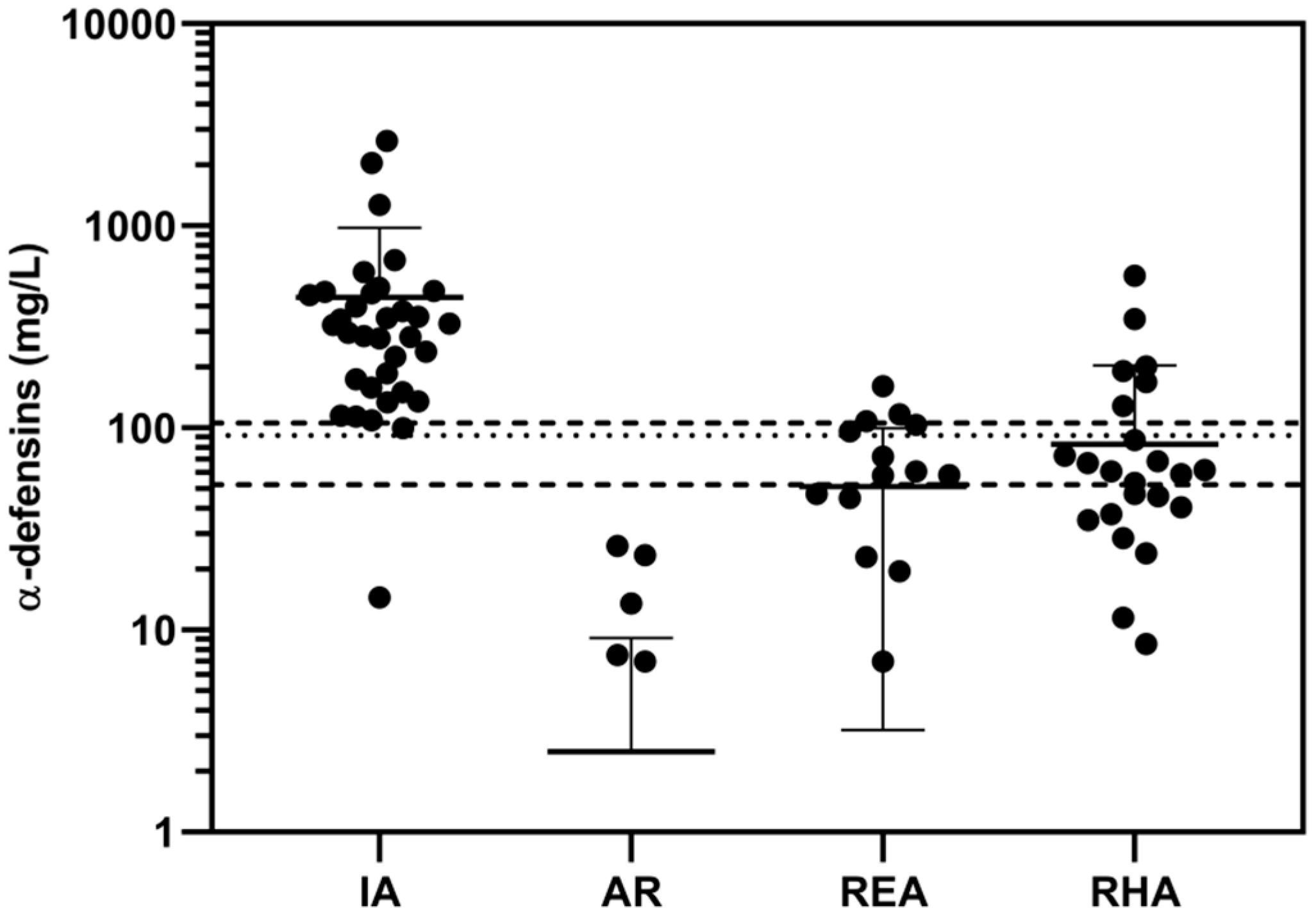
| Cutoff concentration | 5.2 mg/L a, 7.72 mg/L b only for PJI | 5.2 mg/L c only for PJI | 38 mg/L for PJI 98 mg/L for IA |
| Blood in sample | If hemoglobin exceeds 0.5 g/dL, result is affected | Does not affect result | Does not affect result d |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melicherčík, P.; Klapková, E.; Kotaška, K.; Jahoda, D.; Landor, I.; Čeřovský, V. High-Performance Liquid Chromatography as a Novel Method for the Determination of α-Defensins in Synovial Fluid for Diagnosis of Orthopedic Infections. Diagnostics 2020, 10, 33. https://doi.org/10.3390/diagnostics10010033
Melicherčík P, Klapková E, Kotaška K, Jahoda D, Landor I, Čeřovský V. High-Performance Liquid Chromatography as a Novel Method for the Determination of α-Defensins in Synovial Fluid for Diagnosis of Orthopedic Infections. Diagnostics. 2020; 10(1):33. https://doi.org/10.3390/diagnostics10010033
Chicago/Turabian StyleMelicherčík, Pavel, Eva Klapková, Karel Kotaška, David Jahoda, Ivan Landor, and Václav Čeřovský. 2020. "High-Performance Liquid Chromatography as a Novel Method for the Determination of α-Defensins in Synovial Fluid for Diagnosis of Orthopedic Infections" Diagnostics 10, no. 1: 33. https://doi.org/10.3390/diagnostics10010033