 Kamila Řasová1*
Kamila Řasová1* Patrícia Martinková2*
Patrícia Martinková2* Michaela Vařejková2
Michaela Vařejková2 Barbora Miznerová1
Barbora Miznerová1 Markéta Pavlíková1
Markéta Pavlíková1 Jana Hlinovská1
Jana Hlinovská1 David Hlinovský3Štěpánka Philippová3
David Hlinovský3Štěpánka Philippová3 Michal Novotný4
Michal Novotný4 Karolína Pospíšilová5
Karolína Pospíšilová5 Paula Biedková1Romana Vojíková1
Paula Biedková1Romana Vojíková1 Jan Havlík4
Jan Havlík4 Valerie Bríd O'Leary6
Valerie Bríd O'Leary6 Marie Černá6
Marie Černá6 Aleš Bartoš7,8
Aleš Bartoš7,8 Tom Philipp1*
Tom Philipp1*- 1Department of Rheumatology and Rehabilitation, Third Faculty of Medicine, Thomayer University Hospital, Charles University, Prague, Czechia
- 2Department of Statistical Modelling, Institute of Computer Science of the Czech Academy of Sciences, Prague, Czechia
- 3Department of Neurology, Third Faculty of Medicine, Thomayer University Hospital, Charles University, Prague, Czechia
- 4Department of Circuit Theory, Faculty of Electrical Engineering, Czech Technical University in Prague, Prague, Czechia
- 5Department of Physical Medicine and Rehabilitation, Military University Hospital Prague, Prague, Czechia
- 6Department of Medical Genetics, Third Faculty of Medicine, Charles University, Prague, Czechia
- 7Department of Neurology, Third Faculty of Medicine, Charles University, Prague, Czechia
- 8University Hospital Kralovske Vinohrady, Prague, Czechia
Introduction: While the role of physiotherapy as part of a comprehensive inpatient rehabilitation is indisputable, clear evidence concerning the effectiveness of different rehabilitation managements [interdisciplinary implementing the International Classification of Functioning, disability and health (ICF) vs. multidisciplinary model] and physiotherapy categories (neuroproprioceptive “facilitation, inhibition” vs. motor/skill acquisitions using technologies) are still lacking. In this study, four kinds of comprehensive inpatient rehabilitation with different management and content of physical therapy will be compared. Moreover, focus will be placed on the identification of novel biological molecules reflective of effective rehabilitation. Long non-coding RNAs (lncRNAs) are transcripts (>200 bps) of limited coding potential, which have recently been recognized as key factors in neuronal signaling pathways in ischemic stroke and as such, may provide a valuable readout of patient recovery and neuroprotection during therapeutic progression.
Methods and analysis: Adults after the first ischemic stroke in an early sub-acute phase with motor disability will be randomly assigned to one of four groups and undergo a 3 weeks comprehensive inpatient rehabilitation of different types: interdisciplinary team work using ICF model as a guide; multidisciplinary teamwork implementing neuroproprioceptive “facilitation and inhibition” physiotherapy; multidisciplinary teamwork implementing technology-based physiotherapy; and standard multidisciplinary teamwork. Primary (the Goal Attainment Scale, the Patient-Reported Outcomes Measurement Information System, and the World Health Organization Disability Assessment Schedule) and secondary (motor, cognitive, psychological, speech and swallowing functions, functional independence) outcomes will be measured. A blood sample will be obtained upon consent (20 mls; representing pre-rehabilitation molecular) before and after the inpatient program. Primary outcomes will be followed up again 3 and 12 months after the end of the program. The overarching aim of this study is to determine the effectiveness of various rehabilitation managements and physiotherapeutic categories implemented by patients post ischemic stroke via analysis of primary, secondary and long non-coding RNA readouts. This clinical trial will offer an innovative approach not previously tested and will provide new complex analysis along with public assessable molecular biological evidence of various rehabilitation methodology for the alleviation of the effects of ischemic stroke.
Clinical trial registration: NCT05323916, https://clinicaltrials.gov/ct2/show/NCT05323916.
Introduction
Ischemic stroke (IS) is one of the leading causes of neurological dysfunction, the most common being motor disability (1) which negatively impacts life quality and active participation (2, 3).
Undoubtedly, complex rehabilitation (4, 5) is needed. Well-coordinated team work is already taken as a standard approach of complex rehabilitation (6). Multidisciplinary management where specialists work in parallel toward addressing problems related to their profession is frequently the case. An interdisciplinary management where specialists are working as a group to achieve a common goal that is explicitly agreed upon using the International Classification of Functioning, Disability and Health (ICF) model recommended by the World Health Organization (7), is applied rather in Western and Northern European countries, in contrast to other European countries where the use of these tools is rare (8). No study comparing the effectiveness of an interdisciplinary teamwork implementing the ICF model with multidisciplinary teamwork in stroke (7, 9) has been carried out so far.
Physiotherapy (PT) as a part of the team rehabilitation work plays an indisputable role in impairment reduction, activity independence, social participation and quality-of-life improvement (5). Many PT techniques have been developed to facilitate the recovery of motor disability in patients after stroke (1, 6, 10, 11). Clear evidence about what kind of PT approaches as part of rehabilitation is more effective is still missing (12). Several studies compared different PT methods (13), but only small beneficial differences between groups were found probably due to a-systematic/accidental indication of PT methods in rehabilitation processes (14, 15). This is a reason why we decided to compare an effectiveness of main PT categories, 1. motor/skill acquisitions using technologies and 2. neuroproprioceptive “facilitation, inhibition” (16). Both are related to plasticity (the capacity of the central nervous system to adapt and change) via the development of new neuronal interconnections, acquiring new functions, and compensating for impairment (17). In Motor/skill acquisitions using technologies, the patient is increasingly active in the motor re-training process and the principles of sensory-motor learning are applied. Such approach induces a cortical network reorganization closely related topographically to the trained movement which leads to synaptogenesis (18). In neuroproprioceptive ′facilitation, inhibition′ PT, the effectiveness of the synaptic connections among neurons forming functional networks is enhancing with aim to evoke the movement by a suitable combination of afferent stimuli. It modulates interneuronal systems, repeatedly activates motor programs at the subcortical level, and as such induces adaptive and plastic processes of the CNS (19). Until now, nobody compared an effectiveness of these two PT categories which use different mechanisms to activate processes of the plasticity. The only comparison of technology-based PT with equal intensity of over-ground rehabilitation did not show superiority of one over the other (20).
One of the most used options to investigate adaptive and plastic processes of the CNS are imaging methods as functional magnetic resonance or diffusion tensor imaging. Unfortunately, localization and size of changes following rehabilitation are dynamic and differ between studies (21). Research in other areas suggests that molecular biomarkers could be indicators of improvements in neurobiological principles that support repair or compensatory strategies that stimulate adaptive responses in people after stroke (22). The role of long non-coding RNA (lncRNA), defined as RNA transcripts >200 nucleotides with limited coding potential (23), e.g., MALAT1, SNHG12, MEG3 and H19, in ameliorating IS brain injury has now been recognized (24). FosDT might be an important lncRNA for modulation of ischemic neuronal damage, and the inhibition of lncRNA H19 protected cells from OGD/R-induced death by preventing autophagy activation (25). Long non-coding RNA are pivotal factors in neuronal repair processes and enhance neurogenesis. Nevertheless, there is a lack of human studies and clinical trials involving lncRNAs in IS treatment. The medical community has stressed the urgency of implementing studies that may clarify the clinical impact of lncRNAs in the specific context of IS given their promising involvement in nervous system recovery. They have been classified into anti-sense, intronic, large intergenic, promoter associated and UTR-associated lncRNAs (26). They are involved in vital cellular regulation (27) including genomic imprinting (28), epigenetic chromatin modification (29), transcriptional interference (30) and nuclear export (31). Importantly, lncRNAs determine nervous system development (32). A majority of lncRNA display specific expression within neuroanatomical regions (33). Many of these lncRNAs display genomic localizations in close proximity to known neurodevelopmental regulators (34). This has led to the general hypothesis that the expanded diversity in lncRNAs is pivotal to the higher order cognitive ability of humans. LncRNAs regulate key factors involved in ischemic/reperfusion injury, e.g., calcium overload. Excessive calcium accumulation results in the activation of calcium/calmodulin-dependent protein kinase II (CaMKII), a family of serine/threonine kinases involved in IS pathogenesis (35). CaMKII is controlled by lncRNA C2dat1. Elevated levels of lncRNA C2dat1 have been identified in both in vitro and in vivo models of IS (35). The lncRNA CAMK2D-associated transcript (C2dat1) is able to regulate CaMKIIδ, a CaMKII isoform, by targeting CAMK2D-associated transcript (C2dat1), thus being able to regulate key factors involved in I/R injury such as calcium overload or glutamate toxicity, and C2dat1 promoted neuronal survival via activation of nuclear factor kappa B (NF-κB) signaling cascade, which may suggest C2dat1 is a promising therapeutic approach for ischemia. On the other hand, another report showed that the inhibition of CaMKII can prevent 30–70% of ischemia-induced neuronal death; respectively, the regulation of lncRNAs may exert pro-angiogenic, neuroregenerative, anti-apoptotic, and anti-inflammatory effects in injured brain tissue (24). Studies showed that IS injury leads to increased glutamate release activating N-methyl-D-aspartate (NMDA) receptors which initiate cellular apoptosis (36). Overexpression of lncRNA GAS5 increased the apoptotic rate in neurons with its administration resulting in a greater area of cerebral infarction in animal models (37). It has been suggested that inhibition of the lncRNA GAS5 could potentially reduce apoptosis and infarct size in IS leading to improved neurological functioning. Evidence has pointed to lncRNA moderation of autophagy, angiogenesis and oxidative stress caused by IS. Exploring lncRNAs involved in such processes may assist in understanding the recovery networks induced by IS rehabilitation approaches.
For association analysis which may provide further evidence identifying indicators of effective rehabilitation, systematic collection of demographics, clinical and molecular marker information is important. Until now, there is limited evidence to guide judgements regarding the rehabilitation potential following stroke (24, 38–41). An intensity of rehabilitation program appears to be one the most suitable predictor of its effectivity (40, 42), but it is unclear if high intensity programs such as the intensive comprehensive program with a minimum duration of 4 h a day recommended by the Czech Ministry of Health (43) is beneficial or all patients. However, there is limited evidence, whether such intensive program is more effective than the comprehensive rehabilitation program standardly offered. Research also shows that some clinical features such as the level of consciousness, severity of hemiplegia, incontinence, dysphagia and dysphasia (44) or disease severity (45, 46) may be considered as indicators as to whether the rehabilitation process could be effective, however, there exists a certain amount of confusion between predicting natural unassisted recovery and predicting responsiveness to targeted rehabilitation (38).
The current clinical trial aims at filling the above-mentioned research gaps in effectiveness of rehabilitation after stroke. The primary aim is to compare the effectiveness of an interdisciplinary teamwork implementing the ICF model with multidisciplinary teamwork in stroke. As the next aim, we are interested whether PT using principles of sensorimotor learning implementing technology is more effective than neuroproprioceptive “facilitation, inhibition” PT. We focus on PT categories instead of on specific intervention methods, however, information about specific intervention (e.g., Bobath concept, Vojta reflex locomotion) each patient underwent will be recorded and included in the analysis. As the third aim, we focus on the identification of novel biologicals reflective of effective rehabilitation by molecular assessment, in order to answer the question whether the long non-coding RNA is a suitable biomarker for documenting the plastic and adaptive processes of the CNS. Finally, using a uniquely complex dataset, we aim to research what factors play role in effective post stroke rehabilitation and which clinical tests and scales are the most useful in documenting effectiveness of the rehabilitation, even from a long-term perspective.
This clinical trial will test the following scientific hypotheses:
I. COMIRESTROKE under all four settings has a positive influence on all measured outcomes, both in short- and in the long-term. Intensive complex rehabilitation (COMIRESTROKE ICF, NEFI, TECH) has higher effect on all outcomes than standard complex rehabilitation (COMIRESTROKE control).
II. Interdisciplinary management implementing ICF model (COMIRESTROKE ICF) has higher effect than multidisciplinary management (COMIRESTROKE NEFI. TECH, CONTROL) on primary outcomes (GAS, PROMIS, WHODAS 2.0) and on such secondary outcomes that were identified as treatment goals for individual patient. Furthermore, we expect the highest impact on the primary outcomes in the follow-up (three and 12 months after finishing rehabilitation).
III. COMIRESTROKE—NEFI has higher effect than COMIRESTROKE—TECH on the secondary outcomes, mainly on motor functions. Moreover, it leads to the stronger initiation of plastic and adaptive processes, as assessed by the level of lncRNAs in the peripheral blood.
IV. Changes in molecular biological readouts will correlate with changes in clinical parameters and will be the most sensitive to document effect of the therapy.
V. The most important predictor of effective rehabilitation is the level of disability at admission time. However, the category of the rehabilitation has an impact on perceived, clinical, and physiological changes of the rehabilitant.
Moreover, we have these two additional exploratory goals:
Goal I—Improvement patterns: Considering the high number of measured outcomes, for a deeper understanding of therapy efficacy with respect to patient and treatment characteristics, this clinical trial will aim to identify groups of patients with similar improvement patterns post therapy.
Goal II—Item-level analysis: To provide a deeper understanding of the differences in effectiveness between the three therapeutic approaches, this clinical trial aims to explore item-level between-group differences in improvement.
Research from other areas also suggests that between-group differences in improvement may be found on an item level of multi-item measurements even in cases when they are not observed on the total scores, and thus, a more detailed item-level analysis may provide an important insight.
Methods and analysis
Study design
This will be a Four-Arm Parallel-Group Randomized Double Blinded Controlled Trial with a longitudinal design. Patients who fulfilled inclusion criteria will be randomly assigned to one of four research groups (Group 1, 2, 3, or 4). Participants will be examined four times (Figure 1). Primary and secondary outcomes will be measured, and a blood sample will be obtained before and after the inpatient program. Primary outcomes and a blood sample will be followed up again 3 and 12 months after the end of the program (Table 1).
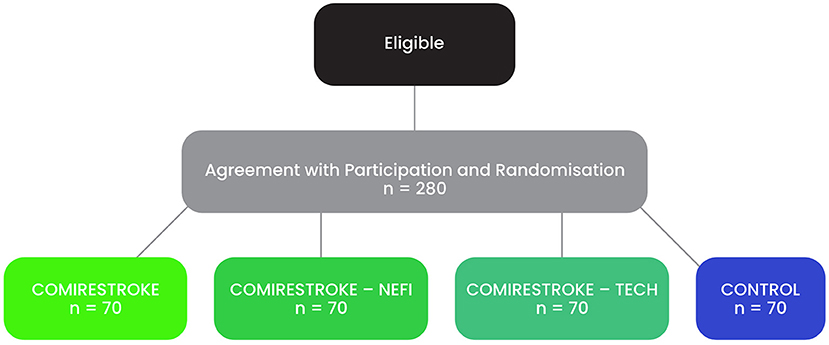
Figure 1. Study design.
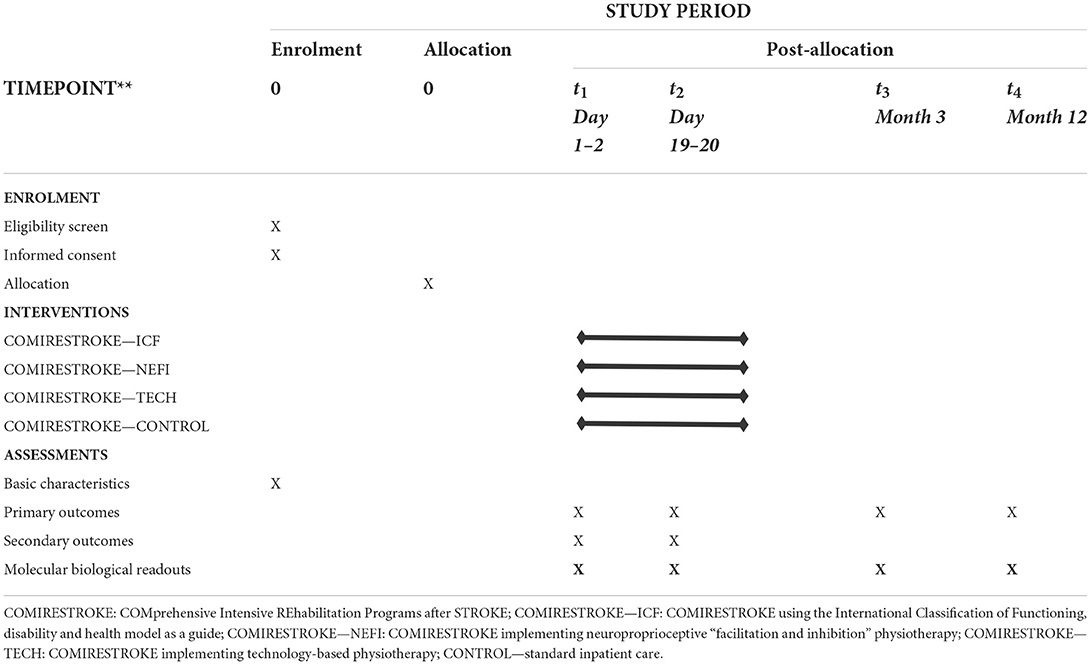
Table 1. Study design.
The SPIRIT reporting guidelines were used when developing the protocol (47). Moreover, recommendation of the Czech Ministry of Health (43) influenced the protocol in (1) the definition of the rehabilitation intensity in interventions cohorts COMIRESTROKE ICF + NEFI + TECH (minimally 4 h of rehabilitation per day), (2) the choice of methods for comprehensive clinical testing, and (3) implementation of technology-based PT. Our department wanted to improve clinical care about people after stroke and decided to implement this best practice. While preparing a clinical project based on this document (43), our scientifically unresolved questions, that we presented in the introduction, we encountered.
Participants
Participants will be identified by a neurologist based on inclusion criteria: Adults (18–85 years) after the first IS in early sub-acute phase, specifically 7 days-3 months (48, 49)—phase the most important for recovery involving spontaneous improvement as well as benefits arising from previous therapeutic intervention (11), with a slight to moderately severe disability {2–4 on the Modified Rankin Scale (50)}, with minimal or moderate motor deficit of upper or lower extremities (on NIHSS Item 5 or 6 scores 1–3 points) who were able to perform activities of daily living prior to stroke event {0–2 on the Pre-Stroke Modified Rankin Score (51)}, with a potential to accept 4 h of comprehensive rehabilitation per day and to profit from the physiotherapy. Czech is their native language or its knowledge is at the level of the mother tongue.
Exclusion criteria
Low level of consciousness (vegetative state and/or minimally conscious state); severe cognitive decline that would interfere with administration of the tests, premorbid illiteracy, severe visual and/or auditory deficit that would prevent proper completion of the tests; behavioral disorders and/or lack of cooperation with therapist; and severe medical problems with a poor prognosis (e.g., severe frailty, advanced and incurable cancer, fracture, cardiovascular disorders as chronic heart failure NYHA III, IV, symptomatic coronary artery disease, angina severity class III, IV, respiratory insufficiency as chronic obstructive pulmonary disease GOLD IV, and another severe disease) (52).
Randomization
All patients meeting the above criteria will be invited to participate and asked to provide a written informed consent. They will be randomly assigned (1:1:1:1) as soon as possible, but always within 48 h of admission, into one of the four interventions (represented by Group 1, 2, 3 or 4) using offsite-independent randomization protocols (www.randomization.com). Concealed allocation will be performed using sequentially numbered opaque sealed envelopes only accessible by research personnel with no involvement in the trial.
Estimated size
It is estimated that ~140 people will be recruited to the clinical trial each year. This number is based on the fulfillment of performance and quality indicators report of cerebrovascular care at the Center for Highly Specialized Patient Care for Stroke Patients at Thomayer Hospital 2019. A total of 280 people is expected to be enrolled in the clinical trial over a period of 2 years (Figure 2), corresponding to a sample number of 70 patients per group. This is sufficient to detect a difference between two groups with the effect size of 0.5 (Cohen's d, considered as moderate to large effect), a significance level of α = 0.05 and a strength of 1-β = 0.80. To detect the effect of therapy within group, required sample size would be even lower as paired t-test will be used. Considering an effect size of 0.5 for WHODAS 2.0 scores is appropriate according to previous studies (53).

Figure 2. Planned Recruitment and Randomization Process.
Interventions
All participants will undergo a complex 3 weeks inpatient rehabilitation. Group 1, 2, 3 undergo intensive rehabilitation (4 h/day for 3 weeks) while intensity in group 4 will be defined by medical doctor (standard procedure). Management of Group 1 will be interdisciplinary, implementing ICF model, while in Group 2, 3 and 4 will be multidisciplinary managed. PT in group 2 will be based on principles of neuroproprioceptive “facilitation inhibition” and in Group 3 based on sensorimotor learning (motor/skill acquisition using technologies) while content of group 4 will not be pre-defined, but it will be indicated by the medical doctor (Table 2).
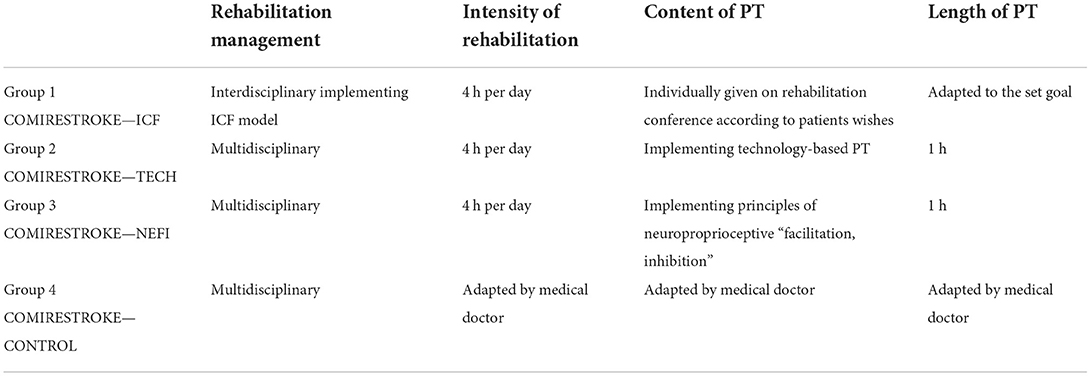
Table 2. Main differences in the intervention between four groups.
Therapists in each group will be maximally helpful and will adopt a schedule for each patient to complete all the sessions. The treatment in each session will be led in person by well-educated, experienced therapists especially trained in each method. Rehabilitation team working with cohort 1 underwent 2 days on-line worskhop (54) and work under supervision of Czech specialist in the ICF concept (55).
The treatment will be modified according to the patient's status and reaction to the therapy. Physical load during all therapies will be perceived maximally as a moderate level of intensity {12 on the Borg Scale (56)}. Information about the treatment (frequency, length and content of each treatment session) will be recorded using codes of Public Health Insurance, Czech Republic (codes correspond to The Current Procedural Terminology code set system) (Table 3). Moreover, content of PT will be defined using Vocabulary of PT interventions (16).
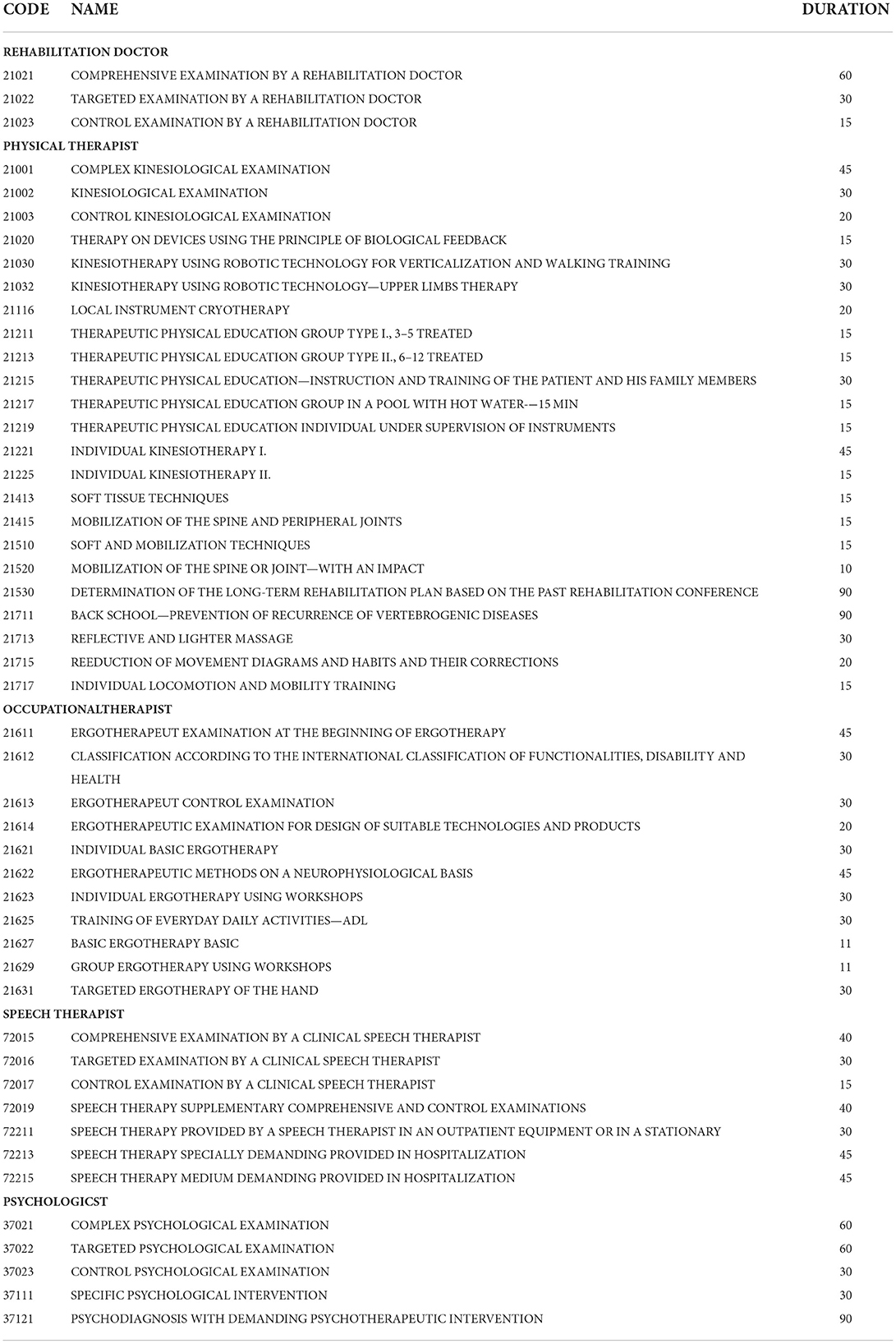
Table 3. Information about the treatment.
Group 1: COMIRESTROKE—ICF (interdisciplinary team management implementing ICF system)
Participants will undergo intensive (4 h per day) rehabilitation where the interdisciplinary team of professionals from different clinical fields (physiotherapy, occupational therapy, clinical speech therapy and psychology) will co-operate using the ICF management tools (such as the ICF Intervention Table, defining and modifying therapeutic interventions in respect to the paitent's goals and sub-goals and in concordance with the functional profile agreed on rehabilitation conferences). These ICF tools are used for systematic organization of the interdisciplinary team.
First therapeutic day, a functional profile will be created by interdisciplinary team and rehabilitator on rehabilitation conference to take into account the functioning, activity and participation level of the patient (57–59).
In order to limit the burden of repetitive clinical examinations, questionnaires surveys and completion of documentation, this study proposes direct linking of some normal-range clinical test results to the codes included in the Comprehensive ICF Stroke Brief set (60) and Rehabilitation set (ICF 30 generic set) (61) (Table 4).
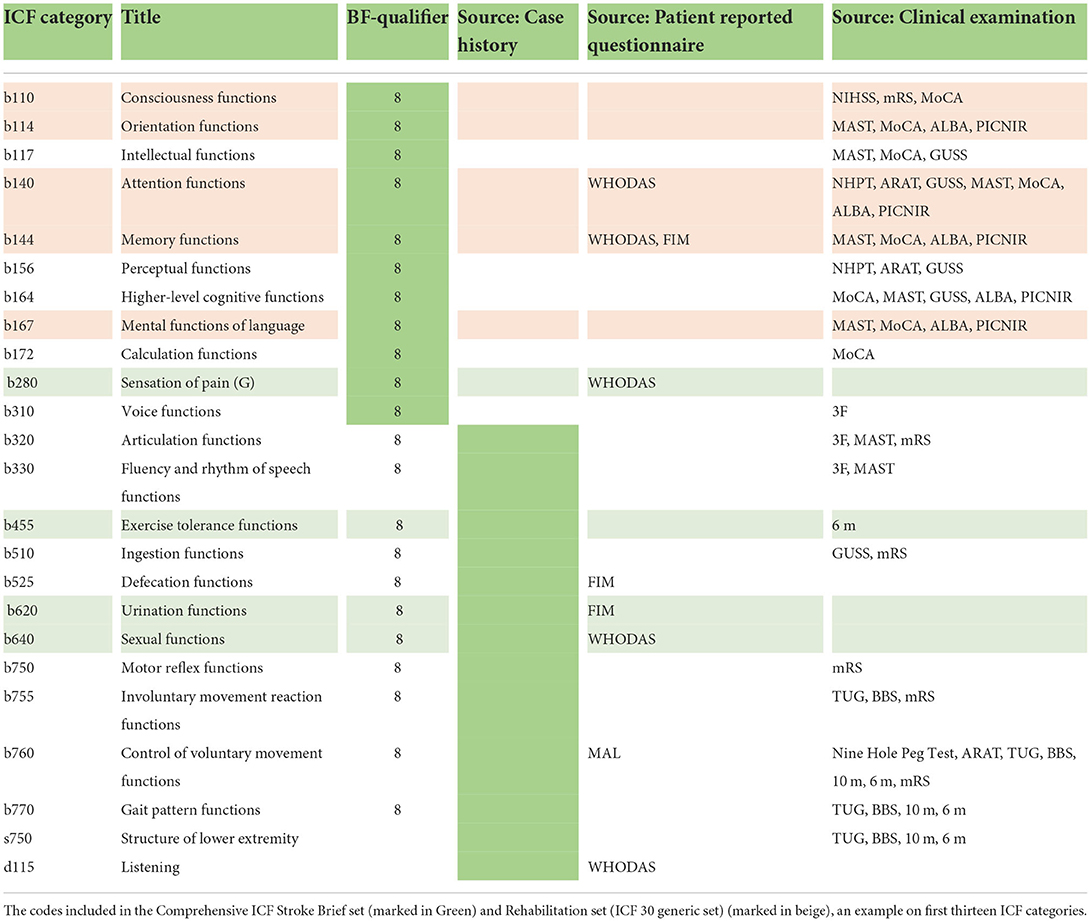
Table 4. An example of linking of clinical test results to the codes.
The interdisciplinary team together with the patient will use the functional profile to define in detail the overall goal and sub-goals of the treatment (62, 63), and to determine specific therapeutic interventions to achieve them (42).
The whole team will work on defined goals, so the time spent with each specialist will depend on the individually set goals. An “ICF Intervention Table” (64) will be used to monitor and evaluate the work during individual targeted interventions and will also serve as a means of communication between the members of the interdisciplinary team. Length of PT will be adapted to the set goal. If the patient wishes to improve some motor skill, it will be longer than if he wishes to improve, for example, speech.
The team will meet weekly (every Monday) on rehabilitation conference to provide feedback, evaluate the fulfillment of the set goals and to adjust therapeutic procedures so that the goals of the therapy are best met.
After finishing hospitalization, participants will undergo a 1-month outpatient rehabilitation programme based on the ICF concept and later will receive standard health and social care.
Group 2: COMIRESTROKE—TECH (motor/skill acquisition implementing technology-based PT)
Participants will undergo intensive (4 h per day) rehabilitation where the multidisciplinary team of practitioners from different clinical fields (physiotherapy, occupational therapy, clinical speech therapy and psychology) will be led by a medical doctor, a specialist in rehabilitation and physical medicine.
One therapeutic intervention (60 min) will be pre-defined as individual PT using principles of sensorimotor learning, i.e., repeated specific and targeted functions in different environments/conditions in order to learn trained motor function, strengthen memory footprint for this function, and as such to initiate plastic and adaptive processes in the CNS. According to the motor function indicated by PT to learn (for example walking or drinking), the most appropriate technology will be chosen, for example robotic systems using an exoskeleton (Gloreha, Erigo and Meditutor) or a therapy applied in virtual environment (65, 66).
After finishing hospitalization, participants will undergo standard/not directed treatment offered by the Czech Health Care system.
Group 3: COMIRESTROKE—NEFI (PT implementing neuroproprioceptive “facilitation, inhibition”)
Participants will undergo intensive (4 h per day) rehabilitation where the multidisciplinary team of practitioners from different clinical fields (physiotherapy, occupational therapy, clinical speech therapy and psychology) will be led by a medical doctor, a specialist in rehabilitation and physical medicine.
One therapeutic intervention (60 min) will be pre-defined as individual PT based on principles of neuroproprioceptive “facilitation, inhibition” PT, it means methods like Vojta reflex locomotion (67), Bobath concept (68), Proprioceptive Neuromuscular Facilitation (61), Motor Program Activating Therapy (69), etc. All these methods apply the appropriate stimuli in different postural positions in order to activate optimal motor function and ability control. They modulate neuronal threshold, and as such induces adaptive and plastic processes of the CNS.
After finishing hospitalization, participants will undergo standard/not directed treatment offered by the Czech Health Care system.
Group 4: COMIRESTROKE—CONTROL
Participants will undergo standard multidisciplinary care including face to face physiotherapy (bed mobility, transfers, gait, therapeutic exercises, positioning, education) recommended by medical doctor.
After finishing hospitalization, participants will undergo standard/not directed treatment offered by the Czech Health Care system.
Pre- and post-intervention assessments
Once an informed consent is obtained prior to randomization; participants will be referred to study examiners—a physical medicine and rehabilitation physician, a neurologist, a physical therapist, a speech therapist, an occupational therapist and a psychologist, who will not know the treatment group of the patient. They will administer baseline testing during the 2nd and 3rd day after admission to the department (Pre-assessment). Post-assessment 1 will be done at the end of the 3-week inpatient intensive comprehensive rehabilitation (during the last 2 days of hospitalization). Follow-up assessments will take place 3 and 12 months after admission, respectively, by a telephone interview or hospital visit. The aim is for each of the measurements to be assessed by a single examiner only (Table 5); in case of more examiners, inter-rater reliability will be assessed.
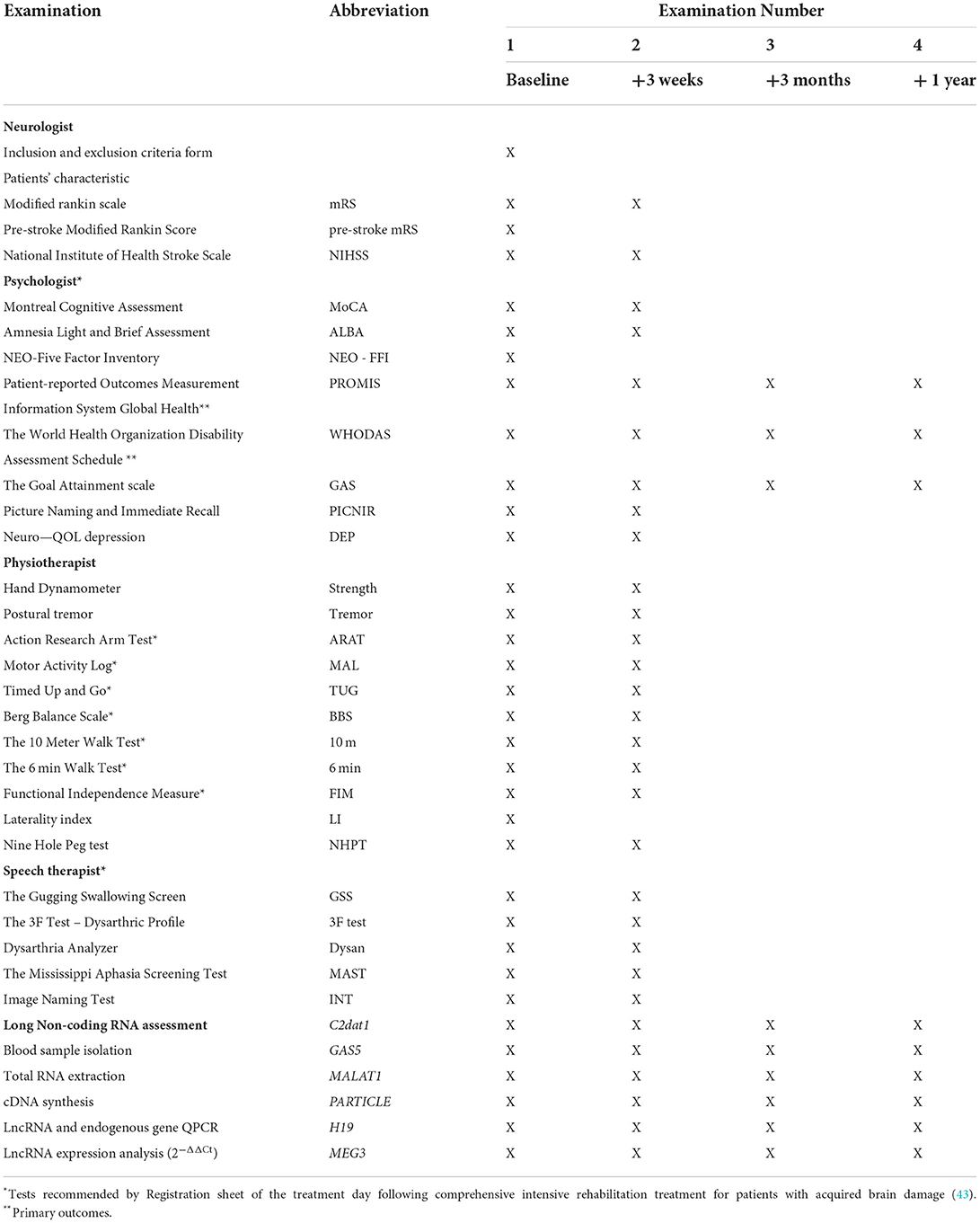
Table 5. Examination timing and distribution by the team.
A wide range of patient characteristics will be collected to address all functions and activities of the patient. To provide systematic categorization (70), the ICF model (6) has been chosen. However, many different measures are used to address different levels of the ICF. Therefore, a team of experienced clinicians and researchers participated in the selection of the most suitable tests into the methodology. Choosing was influenced by psychometric properties, appropriateness of the instrument, but also by use of test in specific regional contexts (71).
We considered the patients' subjective feelings about how they have improved to be the most important aspect. Therefore, the Goal Attainment scale (GAS) together with the Patient-Reported Outcomes Measurement Information System (PROMIS) Global Health, and the World Health Organization Disability Assessment Schedule (WHODAS 2.0) have been chosen as primary outcomes. As secondary outcomes, motor, cognitive, psychological, speech and swallowing functions as well as functional independence will be measured. When choosing secondary outcomes, we based on recommendation of Czech Ministry of Health (43). In this document, list of recommended tests for physical therapists and occupational therapists was presented. Specifically, Action Research Arm Test, Motor Activity Log, Timed Up and Go, Berg Balance Scale, The 10 Meter Walk Test, The 6 Min Walk Test and Functional Independence Measure. They have been supplemented by objective examinations like Nine Hole Peg Test, the Hand Dynamometer and Accelerometer (72) which may provide more extensive information. Assessment of clinical psychologists and speech therapists was not defined in this recommendation and was chosen by expert consensus.
Demographic and anamnestic data including personal factors (sex, age, education, occupation, social relations, living situation), weight and height, laterality index (73), number of days after the stroke event, personality based on the NEO-Five Factor Inventory (NEO-FFI) (74), pre-stroke functional status based on modified Rankin Scale (75), cardiovascular risk factors (76), the degree of neurological impairment according to the National Institute of Health Stroke Scale (77) and disability with the Modified Rankin Scale (50), Bamford classification of IS based on the initial presenting symptoms and clinical signs (78) as well as pharmacotherapy will be collected.
Primary outcomes
As primary outcomes, scales documenting the patients' subjective feelings about how they have improved will be be chosen.
• PROMIS Global Health is a 10-item scale which asks the patient to assess (self-report) their physical, mental and social health in the past 7 days (79, 80).
• WHODAS 2.0 is a generic assessment instrument developed by WHO to provide a standardized method for measuring health and disability. It is grounded in the conceptual framework of the ICF and integrates an individual's level of functioning in major life domains and directly corresponds with ICF's “activity and participation” dimensions. The 36-item version will be used. A higher score means greater disability (81).
• GAS is an individualized outcome measure involving goal selection and goal scaling that is standardized in order to calculate the extent to which a patient's goals are met. Each goal is rated on a 5-point scale (-2 much less than expected, 0 achieved the expected level, 2 much more than expected (82, 83).
Three types of goals will be established:
A. Overarching long-term goal (Global Goal, G) that reflects a desired improvement on the level of participation: usually restoration of previous life including remunerative employment, sport and leisure activities (interview by call at 3 and 12 months follow up).
B. Mid-term goal (Program Goal, P) that reflects improvement mainly in the domain of activities and participations achievable by the rehabilitation program: restoration of self-care (almost), independence in daily living, etc. (interview by call at 3 months follow up).
C. Three Short-term goals (Cycle Goals C1, C2, C3) mainly in the domain of functioning and activities. Usually specific, most problematic components of the Program Goal (evaluated by the rehabilitation team together with the rehabilitant).
The secondary outcomes
The secondary outcomes include clinical tests and questionnaires of physical functions and functional independence (examined by a physical therapist), speech and swallowing (examined by a speech therapist), cognitive and psychological functions (examined by a clinical psychologist).
Upper extremity functions
Jamar Hydraulic Hand Dynamometer will be used to measure isometric grip force from 0 to 90 kg. Five handle positions from 35 to 87 mm will be tested. The measurement is in kg (the higher the value, the better the function) (84).
A postural tremor will be measured by the 3-axis accelerometer and 3-axis gyroscope chip (Motion Tracking sensor MPU-6050) which can measure acceleration up to 16 g and rotation up to 2,000 degrees per second. The sensor will be fixed to the patient using a ring on a finger during stretching the whole arm forward, separately passed for the left and right hand and with opened and closed eyes (1-min measurement for each position). Data from the chip will be acquired by an own measuring device with microcontroller Atmel Mega 328 and stored on an SD card.
For the signal analysis, the magnitude of acceleration—the root of the sum of each component squared—will be computed from separate axes. The sampling frequency will be 100 Hz. Thus, four signals with 6,000 samples will be recorded for each patient—records of postural tremor for right/left hand with opened/closed eyes.
For each record, the signal of acceleration will be filtered by a filter of isoline (typically by high-pass 2nd order Butterworth filter with cut-off frequency of 0.5 Hz). Consequently, the power spectral density (PSD) will be estimated.
The spectral characteristic will be parameterized by selected parameters, for example fMAX (a frequency for which the smoothed PSD is maximal—lower value, lower tremor) or Pf1–f2 (a power of the signal in band from f1 to f2—lower value, lower tremor) (72).
Nine Hole Peg Test is used to measure finger dexterity. A client takes the pegs from a container, one by one, and places them into the holes on the board, as quickly as possible. Shorter times reflect better functioning (85).
Action Research Arm Test (ARAT) is a 19 item observational measure to assess upper extremity performance (coordination, dexterity and functioning). Items are categorized into four subscales (grasp, grip, pinch and gross movement). A higher score means better functioning (86).
Motor Activity Log is a scripted, structured interview to measure real-world upper extremity function consisted of 14 activities of daily living such as using a towel, brushing teeth, and picking up a glass. A higher score means better functioning (87).
Mobility and walking
Timed Up and Go is a simple performance-based measure of dynamic balance. The subject stands up from a chair, walks 3 meters, turns back, and sits down again as quickly and safely as possible while being timed. Shorter times reflect better mobility (88).
Berg Balance Scale is a 14-task scale that requires subjects to maintain their balance in positions and tasks of increasing difficulty. A lower score means lower balance capability (89).
The 10 Meter Walk Test is a performance measure used to assess walking speed in meters per second over 10 meters. Shorter time reflects better mobility (90).
The 6 Min Walk Test is a long walking capacity test recording the maximal distance a subject can walk at the fastest speed possible in 6 min. The more distance covered, the better the walking performance (90).
Functional independence
Functional Independence Measure is an 18-item measurement tool which explores an individual's physical, psychological and social function. It uses the level of assistance an individual needs to grade functional status from total independence to total assistance. The higher the score, the greater independence capacity (91).
Speech and swallowing
The Gugging Swallowing Screen is a simple stepwise bedside screen that allows a graded rating with separate evaluations for non-fluid and fluid nutrition starting with non-fluid textures. It assesses the severity of aspiration risk. A higher score means better functioning (91).
The 3F Test—Dysarthric Profile consists of three subtests (Faciokinesis, Phonorespiration, Phonetics). The overall Index of Dysarthria (ID) is a sum of 45 items with the maximum score of 90. A higher score means better functioning (92).
Following previously published guidelines (93), the dysarthria assessment is based on the automatic evaluation of utterances, including sustained phonation, speech diadochokinetic task, and connected speech. Utterances will be recorded during the sessions with speech language pathologist. The recording will take place in a quiet room with low ambient noise using a head-mounted condenser microphone (Shure Beta 53, Niles, Illinois, U.S.), placed ~5 cm from the mouth corner at an angle of 70°. The recordings will be sampled at 48 kHz with 16-bit resolution. The automatic analysis will be performed using the beta version of the freely available Dysarthria Analyzer (Czech Technical University in Prague, available at http://dysan.cz/).
The Mississippi Aphasia Screening Test (MAST) was developed as a brief, repeatable screening measure for individuals with severely impaired communication/language skills. It has nine subtests that range from 1 to 10 items per subscale. The Index scores sum to 50 points each and are added for the MAST Total Score (0–100 points). The higher the score, the better functioning (94).
Image Naming Test (Test pojmenování obrázku, TPO) is a test of confrontational naming of nouns and verbs. Words are selected based on success, frequency of occurrence, age of adoption, length, and visual complexity. The maximum sum is 60 points (30 verbs and 30 nouns), the results can be assessed qualitatively according to the type of unexplained words (95).
Cognitive and psychological functions
The Montreal Cognitive Assessment (MoCA) is an assessment for detecting cognitive impairment ranging from 0 and 30 points. A higher score equates to developed cognition. The Czech version will be validated with cut-offs and norms established (96, 97).
The Amnesia Light and Brief Assessment (ALBA) is an original Czech and innovative test to assess more cognitive functions including short-term memory recall during 3 min. The ALBA consists of four tasks: (1) repetition and encoding of a six-word sentence “Indian Summer Brings First Morning Frost”, (2) sequential demonstration of six gestures, (3) their immediate recall, and (4) final recall of the original sentence. The first task of a sentence repetition reflects (1) language (impaired in aphasia) or (2) encoding and working memory (impaired in memory and attention deficits). The second task of gesturing can be impaired as a result of sensory aphasia or apraxia. Short-term and episodic memory is measured in two different ways, (1) in the third part of the ALBA, i.e., incidental memory of the gestures, and (2) in the fourth part, i.e., intentional verbal memory of the sentence. Overall memory can be expressed as the ALBA memory score, which is a sum of correctly recalled sentence words and gestures. The higher scores of each ALBA part reflect better cognitive functioning. Scores of individual parts range from 0 (the worst) to 6 points (the best) for each of four tasks: (1) the number of correctly repeated words of the sentence (Word 1 score: 0–6 points), (2) the number of correctly recalled words of the sentence after the distraction using the TEGEST (W2 score: 0–6), (3) the number of correctly performed gestures of the TEGEST (Gesture 1 score: 0–6), and (4) the number of correctly recalled gestures of the TEGEST (G2 score: 0–6). The sum, called ALBA memory score, is derived from correctly recalled words of the sentence and correctly recalled gestures together [W2 + G2: 0–12 (6 + 6)]. Example scores of the ALBA test can be the following: 5/1 + 5/3 (W1/2 + G1/2) that gives a total ALBA memory score: 4 (1 + 3) points (98, 99). The ALBA educational video is freely available at: https://www.youtube.com/watch?v=LyCuWc0-Gro.
PICture Naming and Immediate Recall (PICNIR) is an original Czech test certified by the Ministry of Health of the Czech Republic in 2017. The purpose of the PICNIR is to evaluate written speech, long-term sematic and short-term memory simultaneously and quickly up to 5 min. The test consists of two parts. The task of an examinee is to write down names of 20 black and white pictures in one word and remember them at the same time. Then they are asked to rewrite as many picture names as they can recall during 1 min. The results of the PICNIR include a number of wrongly named or unnamed pictures in the first naming part and a number of correctly recalled picture names in the second recall part. The less named errors and more recalled picture names indicate higher cognitive functioning (100). The PICNIR educational video is freely available at: https://www.youtube.com/watch?v=cbJGtPG-nVA.
Neuro–QOL depression is a self-report of health-related quality of life (101).
Other pre-specified outcome measures—molecular biological readouts of rehabilitation
Blood will be taken for total RNA extraction, cDNA synthesis and real-time QPCR assessment of lncRNA candidates previously identified as potential therapeutic influencers in IS. Whole blood will be collected from fasting patients for RNA analysis. A RiboPure™-Blood Kit (cat# AM1928, ThermoFisher Scientific) will be used for isolating high-quality RNA directly from whole blood. This kit contains an RNAlater® Solution (cat.# AM7020, ThermoFisher Scientific) that protects RNA and is designed to eliminate the need to process samples as soon as they are harvested. RNAlater® Solution also “freezes” the gene expression profile of the cells. Treated samples can be safely stored at ambient temperature for extended periods of time (up to 3 days or more). Blood samples stored in RNAlater® Solution yield RNA of comparable quality to blood samples processed directly according to the commercial website. Expected average yields of total RNA will be between 2 and 4 μg/0.5 mL of whole blood. Total RNA will be reverse transcribed into cDNA. Human lncRNA and internal endogenous gene (e.g., GAPDH) expression will be quantified using RNA extracted from blinded samples (i.e., concealment of group allocation) to eliminate bias.
Statistical analysis
Descriptive statistics
On the baseline, the distribution of all primary and secondary outcomes will be visualized using histograms and QQ plots. We expect normal distributions in most of the variables defined as raw scores from appropriate tests, or in their log transformations (e.g., tests measuring time needed to walk certain distance or to perform a task). The groups will be compared in their characteristics, primary, and secondary outcomes using the one-way analysis of variance (ANOVA), and its non-parametric version (Kruskal—Wallis test), where needed. The Benjamini-Hochberg correction (102) will be used to account for multiple comparisons. We expect no differences between groups on the baseline. If differences are observed, these will be accounted for in the longitudinal models.
Measuring the effectiveness of rehabilitation
To test hypothesis I., i.e., a positive influence on all outcomes, the effect of therapy for each therapeutic group will be assessed separately by paired t-tests performed on pre-test and post-test scores. Two sample t-test will be used to compare the patients in the three COMIRESTROKE groups with patients from the control group. The Wilcoxon signed-rank test or Mann-Whitney test will be used on data where normal distribution cannot be expected.
To test hypotheses II. and III, a comparison between therapeutic groups will be performed using two sample Student t-tests on differences between measurement time points (or Mann-Whitney tests, respectively, for data, where normal distribution of the differences cannot be expected). For hypothesis II, the COMIRESTROKE—ICF group will be compared against the participants in other three COMIRESTROKE groups (NEFI, TECH and CONTROL). For hypothesis III, the COMIRESTROKE—NEFI group will be compared against the other three COMIRESTROKE groups (ICF, TECH and CONTROL). A one-sided alternative will be tested according to our hypotheses. We will also implement the one-way ANOVA test to jointly compare all four COMIRESTROKE groups for pre-post differences. In addition, a Tukey post-hoc comparison will be made to detect any further group differences beyond our hypotheses.
To assess the overall impact of rehabilitation and to compare effectiveness of different therapeutic approaches for Hypotheses I—III in more complex way, and to test for effect of other covariates in Hypothesis V, a linear mixed effect model will be used with random patient effect fitted to longitudinal patient data. Measurement effect, group effect and their interaction, as well as effects of other covariates such as the level of disability in admission time will be tested by F-test.
To address Hypothesis IV and Exploratory Goal I, correlations between changes in different examination scores will be evaluated using Pearson correlation coefficient and its non-parametric analogies. A cluster analysis will be performed to identify different phenotypes. This will allow the identification of different groups of patients in relation to the efficacy of the neuro-rehabilitation programs.
To address Goal II, for selected multi-item instruments, item-response theory (IRT) and generalized linear regression models will be used to study differential item functioning with respect to rehabilitation groups. Account will be taken for other respondent characteristics. Use will be made of differential item functioning in change (DIF-C) analysis (7) in order to detect between-group differences.
Statistical software
Analysis will be performed using the free statistical environment R (103) and its libraries. The lme (104) and nlme (105) library will be used for implementing mixed effect models. Library difNLR (106) will be used for the detection of DIF. Modules of the interactive ShinyItemAnalysis application will enable lme (104), nlme (105) and difNLR (106) library sample analyses to be interactively displayed (107).
Data monitoring
Data quality will be monitored by an independent person within 2 days after each set of assessments (pre, post, follow-up) is completed. An interim data analysis will be conducted by an independent data analyst each month or after data from at least 10 new patients are collected. The trial will be terminated when planned number of participants (n = 280) is collected.
Harms
This study poses no greater risks than standard care. Examinations will be carried out by competent examiners and therapy by qualified specialists. The program might be customized to prevent patient's exertion, although that is not anticipated, since the level of exercise load should be mild.
We do not expect adverse events which could cause trial termination. Any potential adverse events will be reported in https://register.clinicaltrials.gov.
Article summary
Strengths and limitations of this study
• This Four-Arm Parallel-Group Randomized Double Blinded Controlled Trial with a longitudinal design will provide evidence of the effectiveness of COMprehensive Intensive REhabilitation Program after STROKE (COMIRESTROKE) on a wide range of primary and secondary outcomes, and long non-coding RNA readouts.
• Comparing different kinds of COMIRESTROKE will provide evidence for on optimal approach to ischemic stroke rehabilitation.
• Blood sampling will assist with offering initial evidence that lncRNAs represent molecular readouts of effective rehabilitation and will provide information about the direct/indirect role of lncRNA in brain neuronal protection before and after COMIRESTROKE.
• The limitation of this study is the difficulty in blinding the treatment from patients.
• Looking for tools regarding the interdisciplinary team management in inpatient care after stroke as well for further feedback, the team has chosen the ICF model and its tools for this purpose. The authors are aware that the ICF model can be used in interdisciplinary, multidisciplinary as well as single-discipline rehab approaches. Coupling the ICF tools with the interdisciplinary rehabilitation management approach in this study is inserting a confounding factor since there may be differences in the effectiveness of interdisciplinary vs. multidisciplinary irrespective of the ICF. This effect must be further studied in future projects comparing the multidisciplinary and interdisciplinary team management approach with/without the ICF tools.
• It is a very large study, the implementation of which depends on good organization of the whole team, both in the neurology and rehabilitation clinics, so control mechanisms must be put in place to avoid data loss.
• A wide range of patient characteristics will be collected. To avoid overburdening patients, the examination will be effectively organized over 2 days. Additionally, examination by a clinical psychologist and speech therapist will be done in such a way as to bring a therapeutic effect.
• One of the most important outputs of this clinical trial will be the recommendation concerning which clinical tests and scales are the most useful in post-stroke rehabilitation based on the framework of the ICF model. This finding will only apply to tests selected for our protocol that was influenced by recommendation of Czech Ministry of Health, and as such may not be applicable generally.
• As in clinical practice, multi-item measurements are used to guide rehabilitation programs, we consider that an item-level analysis may provide a deeper insight into the effectiveness of different interventions.
• The development of the protocol was influenced by the health care organization in the Czech Republic where multidisciplinary team management prevails and PT category neuroproprioceptive “facilitation, inhibition” is predominantly used/applied. Therefore, the results of the study may not be applicable in other healthcare systems.
• In conclusion, the proposed study will determine the effectiveness of COMprehensive Intensive REhabilitation Programs after STROKE involving various approaches of management (interdisciplinary team work implementing individualized rehabilitation using the International Classification of Functioning, disability and health model as a guide with multidisciplinary team work) and physical therapy categories (neuroproprioceptive “facilitation and inhibition” physical therapy and motor/skill acquisition implementing technology-based physical therapy) via analysis of primary, secondary and lncRNA readouts.
• This clinical trial will offer an innovative approach not previously tested and will provide new complex analysis along with public assessable molecular biological evidence of various rehabilitation methodologies for the alleviation of the effects of ischemic stroke.
Ethics and dissemination
The Ethical committee of the Institute for the Clinical and Experimental Medicine and Thomayer University Hospital have approved the study under number 09306/22 (6-21_01). Written, informed consent to participate and provide blood samples will be obtained from all participants (information for participants and inform consent are available at in https://register.clinicaltrials.gov). Protocol amendments are not expected, but in case that any amendments are needed, such amendments will be subject to approval by The Ethical committee of the Institute for the Clinical and Experimental Medicine and Thomayer University Hospital.
Personal information will be collected, shared, and maintained in order to protect confidentiality according to valid laws of the Czech Republic before, during, and after the trial. Access to the dataset will be given to independent data analysts and will be limited for investigators. Participation in the study has a minimum of known risks, however, in the event of any damage to the study participant related to his/her participation in the project, this person will be compensated by hospital insurance. Study results will be published in journal articles and reported on https://register.clinicaltrials.gov. Anonymized data will be disseminated via https://osf.io or other data sharing platforms, anonymized lncRNA expression data will be uploaded onto Genbank and made freely available to the scientific community.
The current approved version of the protocol NCT05323916 is version released 04/27/2022. The trial has yet not commenced. First patient enrolment is planned for May 2022. Recruitment will be completed by December 2025.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Committee of the Institute for the Clinical and Experimental Medicine and Thomayer University Hospital. The patients/participants provided their written informed consent to participate in this study.
Author contributions
KŘ, PM, MP, BM, and TP: conceptualization. KŘ and TP: resources. KŘ, VO'L, and PM: writing-original draft preparation. KŘ, PM, MV, BM, MP, JHl, DH, ŠP, MN, KP, PB, RV, JHa, VO'L, MČ, AB, and TP: writing—review and editing. KŘ, PM, KP, and JHa: project administration. All authors: methodology and electronic case report form. All authors have read and agreed to the published version of the manuscript.
Funding
Ministry of Health, Czech Republic – RVO (Thomayer University Hospital – FTN, 00064190) supported the development of the design of the study, including payment of license fees and data recording system. PM and MV were supported by the long-term strategic development financing of the Institute of Computer Science (RVO:67985807). JH was supported by the grant no. SGS20/167/OHK3/3T/13 of the Czech Technical University in Prague. The research was also supported by Charles University, programme Cooperatio (Neuroscience and Medical Diagnostics and Basic Medical Sciences, the field ‘Medical Genetics’) and 260533/SVV/2022.
Acknowledgments
We would like to thank Petr Kopsa, MD for coordinating the clinic's work so that we can carry out the research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review. Lancet Neurol. (2009) 8:741–54. doi: 10.1016/S1474-4422(09)70150-4
2. Yagi M, Yasunaga H, Matsui H, Morita K, Fushimi K, Fujimoto M, et al. Impact of rehabilitation on outcomes in patients with ischemic stroke: a nationwide retrospective cohort study in Japan. Stroke. (2017) 48:740–6. doi: 10.1161/STROKEAHA.116.015147
3. Bindawas SM, Vennu V, Moftah E. Improved functions and reduced length of stay after inpatient rehabilitation programs in older adults with stroke: a systematic review and meta-analysis of randomized controlled trials. Neuro Rehabil. (2017) 40:369–90. doi: 10.3233/NRE-161425
4. Bunketorp-Käll L, Lundgren-Nilsson Å, Samuelsson H, Pekny T, Blomvé K, Pekna M, et al. Long-term improvements after multimodal rehabilitation in late phase after stroke: a randomized controlled trial. Stroke. (2017) 48:1916–24. doi: 10.1161/STROKEAHA.116.016433
5. Hopman WM, Verner J. Quality of life during and after inpatient stroke rehabilitation. Stroke. (2003) 34:801–5. doi: 10.1161/01.STR.0000092205.92969.00
6. Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet. (2011) 377:1693–702. doi: 10.1016/S0140-6736(11)60325-5
7. Perin C, Bolis M, Limonta M, Meroni R, Ostasiewicz K, Cornaggia CM, et al. Differences in rehabilitation needs after stroke: a similarity analysis on the ICF core set for stroke. Int J Environ Res Public Health. (2020) 17:4291. doi: 10.3390/ijerph17124291
8. Rasova K, Freeman J, Martinkova P, Pavlikova M, Cattaneo D, Jonsdottir J, et al. The organisation of physiotherapy for people with multiple sclerosis across Europe: a multicentre questionnaire survey. BMC Health Serv Res. (2016) 16:552. doi: 10.1186/s12913-016-1750-6
9. Zhang T, Liu L, Xie R, Peng Y, Wang H, Chen Z, et al. Value of using the international classification of functioning, disability, and health for stroke rehabilitation assessment: a multicenter clinical study. Medicine. (2018) 97:e12802. doi: 10.1097/MD.0000000000012802
10. Brewer L, Horgan F, Hickey A, Williams D. Stroke rehabilitation: recent advances and future therapies. QJM. (2013) 106:11–25. doi: 10.1093/qjmed/hcs174
11. Johansson BB. Current trends in stroke rehabilitation. A review with focus on brain plasticity. Acta Neurol Scand. (2011) 123:147–59. doi: 10.1111/j.1600-0404.2010.01417.x
12. Stinear CM, Lang CE, Zeiler S, Byblow WD. Advances and challenges in stroke rehabilitation. Lancet Neurol. (2020) 19:348–60. doi: 10.1016/S1474-4422(19)30415-6
13. van Vliet PM, Lincoln NB, Foxall A. Comparison of Bobath based and movement science based treatment for stroke: a randomised controlled trial. J Neurol Neurosurg Psychiatry. (2005) 76:503–8. doi: 10.1136/jnnp.2004.040436
14. Martinková P, Drabinová A, Liaw YL, Sanders EA, McFarland JL, Price RM. Checking equity: why differential item functioning analysis should be a routine part of developing conceptual assessments. CBE Life Sci Educ. (2017) 16:rm2. doi: 10.1187/cbe.16-10-0307
15. Martinková P, Hladká A, PotuŽníková E. Is academic tracking related to gains in learning competence? Using propensity score matching and differential item change functioning analysis for better understanding of tracking implications. Learn Instruction. (2020) 66:101286. doi: 10.1016/j.learninstruc.2019.101286
16. Martinková P, Freeman J, Drabinová A, Erosheva E, Cattaneo D, Jonsdottir J, et al. Physiotherapeutic interventions in multiple sclerosis across Europe: Regions and other factors that matter. Mult Scler Relat Disord. (2018) 22:59–67. doi: 10.1016/j.msard.2018.03.005
17. Takeuchi N, Izumi S-I. Rehabilitation with poststroke motor recovery: a review with a focus on neural plasticity. Stroke Res Treat. (2013) 2013:128641. doi: 10.1155/2013/128641
18. Straudi S, Basaglia N. Neuroplasticity-based technologies and interventions for restoring motor functions in multiple sclerosis. Adv Exp Med Biol. (2017) 958:171–85. doi: 10.1007/978-3-319-47861-6_11
19. Rasová K, Bučková B, Prokopiusová T, Procházková M, Angel G, Marková M, et al. A three-arm parallel-group exploratory trial documents balance improvement without much evidence of white matter integrity changes in people with multiple sclerosis following two months ambulatory neuroproprioceptive “facilitation and inhibition” physical therapy. Eur J Phys Rehabil Med. (2021) 6:889–899. doi: 10.23736/S1973-9087.21.06701-0
20. Vaney C, Gattlen B, Lugon-Moulin V, Meichtry A, Hausammann R, Foinant D, et al. Robotic-assisted step training (lokomat) not superior to equal intensity of over-ground rehabilitation in patients with multiple sclerosis. Neurorehabil Neural Repair. (2012) 26:212–21. doi: 10.1177/1545968311425923
21. Matthews PM, Johansen-Berg H, Reddy H. Non-invasive mapping of brain functions and brain recovery: applying lessons from cognitive neuroscience to neurorehabilitation. Restor Neurol Neurosci. (2004) 22:245–60.
22. Johansson BB. Brain plasticity and stroke rehabilitation. Willis Lecture Stroke. (2000) 31:223–30. doi: 10.1161/01.STR.31.1.223
24. Wolska M, Jarosz-Popek J, Junger E, Wicik Z, Porshoor T, Sharif L, et al. Long non-coding RNAs as promising therapeutic approach in ischemic stroke: a comprehensive review. Mol Neurobiol. (2021) 58:1664–82. doi: 10.1007/s12035-020-02206-8
25. Ren W, Yang X. Pathophysiology of long non-coding RNAs in ischemic stroke. Front Mol Neurosci. (2018) 11:96. doi: 10.3389/fnmol.2018.00096
26. Caley DP, Pink RC, Trujillano D, Carter DR. Long noncoding RNAs, chromatin, and development. Sci World J. (2010) 10:90–102. doi: 10.1100/tsw.2010.7
27. Xiao C, Sharp JA, Kawahara M, Davalos AR, Difilippantonio MJ, Hu Y, et al. The XIST noncoding RNA functions independently of BRCA1 in X inactivation. Cell. (2007) 128:977–89. doi: 10.1016/j.cell.2007.01.034
28. Marcho C, Bevilacqua A, Tremblay KD, Mager J. Tissue-specific regulation of Igf2r/Airn imprinting during gastrulation. Epigenetics Chromatin. (2015) 8:10. doi: 10.1186/s13072-015-0003-y
29. O'Leary VB, Hain S, Maugg D, Smida J, Azimzadeh O, Tapio S, et al. Long non-coding RNA PARTICLE bridges histone and DNA methylation. Sci Rep. (2017) 7:1790. doi: 10.1038/s41598-017-01875-1
30. O'Leary VB, Ovsepian SV, Carrascosa LG, Buske FA, Radulovic V, Niyazi M, et al. PARTICLE, a triplex-forming long ncRNA, regulates locus-specific methylation in response to low-dose irradiation. Cell Rep. (2015) 11:474–85. doi: 10.1016/j.celrep.2015.03.043
31. Williams T, Ngo LH, Wickramasinghe VO. Nuclear export of RNA: different sizes, shapes and functions. Semin Cell Dev Biol. (2018) 75:70–7. doi: 10.1016/j.semcdb.2017.08.054
32. Clark BS, Blackshaw S. Understanding the role of lncRNAs in nervous system development. Adv Exp Med Biol. (2017) 1008:253–82. doi: 10.1007/978-981-10-5203-3_9
33. Bechara EG, Didiot MC, Melko M, Davidovic L, Bensaid M, Martin P, et al. A novel function for fragile X mental retardation protein in translational activation. PLoS Biol. (2009) 7:e16. doi: 10.1371/journal.pbio.1000016
34. Castets M, Schaeffer C, Bechara E, Schenck A, Khandjian EW, Luche S, et al. FMRP interferes with the Rac1 pathway and controls actin cytoskeleton dynamics in murine fibroblasts. Hum Mol Genet. (2005) 14:835–44. doi: 10.1093/hmg/ddi077
35. Xu Q, Deng F, Xing Z, Wu Z, Cen B, Xu S, et al. Long non-coding RNA C2dat1 regulates CaMKIIδ expression to promote neuronal survival through the NF-κB signaling pathway following cerebral ischemia. Cell Death Dis. (2016) 7:e2173. doi: 10.1038/cddis.2016.57
36. Ye X, Zhou XJ, Zhang H. Exploring the role of autophagy-related gene 5 (ATG5) yields important insights into autophagy in autoimmune/autoinflammatory diseases. Front Immunol. (2018) 9:2334. doi: 10.3389/fimmu.2018.02334
37. Deng Y, Chen D, Gao F, Lv H, Zhang G, Sun X, et al. Silencing of long non-coding RNA GAS5 suppresses neuron cell apoptosis and nerve injury in ischemic stroke through inhibiting DNMT3B-dependent MAP4K4 methylation. Transl Stroke Res. (2020) 11:950–66. doi: 10.1007/s12975-019-00770-3
38. Enderby P, Pandyan A, Bowen A, Hearnden D, Ashburn A, Conroy P, et al. Accessing rehabilitation after stroke - a guessing game? Disabil Rehabil. (2017) 39:709–13. doi: 10.3109/09638288.2016.1160448
39. Alexander MP. Stroke rehabilitation outcome. A potential use of predictive variables to establish levels of care. Stroke. (1994) 25:128–34. doi: 10.1161/01.STR.25.1.128
40. Shah S, Vanclay F, Cooper B. Efficiency, effectiveness, and duration of stroke rehabilitation. Stroke. (1990) 21:241–6. doi: 10.1161/01.STR.21.2.241
41. Burton CR, Horne M, Woodward-Nutt K, Bowen A, Tyrrell P. What is rehabilitation potential? Development of a theoretical model through the accounts of healthcare professionals working in stroke rehabilitation services. Disabil Rehabil. (2015) 37:1955–60. doi: 10.3109/09638288.2014.991454
42. Hu MH, Hsu SS, Yip PK, Jeng JS, Wang YH. Early and intensive rehabilitation predicts good functional outcomes in patients admitted to the stroke intensive care unit. Disabil Rehabil. (2010) 32:1251–9. doi: 10.3109/09638280903464448
43. MZCR. Registrační List Ošetrovacího Dne Následné Komplexní Intenzivní RehabilitacNí LécBy U Pacientu Se Získaným PošKozením Mozku (Registration Sheet of the Treatment Day Following Comprehensive Intensive Rehabilitation Treatment for Patients With Acquired Brain Damage), REGISTRACNÍ LIST_OD_00033, kranioprogram_MZ CR, Praha, 2020. Praha: MZČR.
44. Feydy A, Carlier R, Roby-Brami A, Bussel B, Cazalis F, Pierot L, et al. Longitudinal study of motor recovery after stroke: recruitment and focusing of brain activation. Stroke. (2002) 33:1610–7. doi: 10.1161/01.STR.0000017100.68294.52
45. Turner-Stokes L. Cost-efficiency of longer-stay rehabilitation programmes: can they provide value for money? Brain Injury. (2007) 21:1015–21. doi: 10.1080/02699050701591445
46. Malhotra S, Pandyan AD, Rosewilliam S, Roffe C, Hermens H. Spasticity and contractures at the wrist after stroke: time course of development and their association with functional recovery of the upper limb. Clin Rehabil. (2011) 25:184–91. doi: 10.1177/0269215510381620
47. Chan A-W, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. (2013) 346:e7586. doi: 10.1136/bmj.e7586
48. Grefkes C, Fink GR. Recovery from stroke: current concepts and future perspectives. Neurol Res Pract. (2020) 2:17. doi: 10.1186/s42466-020-00060-6
49. Bernhardt J, Hayward KS, Kwakkel G, Ward NS, Wolf SL, Borschmann K, et al. Agreed definitions and a shared vision for new standards in stroke recovery research: the stroke recovery and rehabilitation roundtable taskforce. Int J Stroke. (2017) 12:444–50. doi: 10.1177/1747493017711816
50. van Swieten J. Modified Rankin Scale for Neurologic Disability: MDCalc ©. (2021). Available online at: https://www.mdcalc.com/modified-rankin-scale-neurologic-disability#creator-insights (accessed October 22, 2022).
51. American Medical Association. Pre-Stroke Modified Rankin Score (mRS). (2020). Available online at: https://manual.jointcommission.org/releases/TJC2018A/DataElem0569.html (accessed October 22, 2022).
52. Lacas A, Rockwood K. Frailty in primary care: a review of its conceptualization and implications for practice. BMC Med. (2012) 10:4. doi: 10.1186/1741-7015-10-4
53. Ustün TB, Chatterji S, Kostanjsek N, Rehm J, Kennedy C, Epping-Jordan J. et al. Developing the world health organization disability assessment schedule 20. Bull World Health Organ. (2010) 88:815–23. doi: 10.2471/BLT.09.067231
54. Branch, IR. ICF e-Learning Tool. Available online at: https://www.icf-research-branch.org/icf-training/icf-e-learning-tool (accessed October 22, 2022).
55. Angerová Y. Advances in an Inter-Professional Approach to the Examination Rehabilitation of Patients After Brain Injury. (2022). Available online at: https://is.cuni.cz/studium/predmety/index.php?id=e7594df3f7abb1c314d7ca93ddce737f&tid=&do=predmet&kod=DS013 (accessed October 22, 2022).
56. Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. (1982) 14:377–81. doi: 10.1249/00005768-198205000-00012
57. Bukowski L, Bonavolonta M, Keehn MT, Morgan KA. Interdisciplinary roles in stroke care. Nurs Clin North Am. (1986) 21:359–74. doi: 10.1016/S0029-6465(22)00423-6
58. Yagura H, Miyai I, Suzuki T, Yanagihara T. Patients with severe stroke benefit most by interdisciplinary rehabilitation team approach. Cerebrovasc Dis. (2005) 20:258–63. doi: 10.1159/000087708
59. Miller EL, Murray L, Richards L, Zorowitz RD, Bakas T, Clark P, et al. Comprehensive overview of nursing and interdisciplinary rehabilitation care of the stroke patient: a scientific statement from the American heart association. Stroke. (2010) 41:2402–48. doi: 10.1161/STR.0b013e3181e7512b
60. Geyh S, Cieza A, Schouten J, Dickson H, Frommelt P, Omar Z, et al. ICF Core Sets for stroke. J Rehabil Med. (2004) 2004 (Suppl. 44):135–41. doi: 10.1080/16501960410016776
61. Prodinger B, Reinhardt JD, Selb M, Stucki G, Yan T, Zhang X, et al. Towards system-wide implementation of the international classification of functioning, disability and health (ICF) in routine practice: developing simple, intuitive descriptions of ICF categories in the ICF generic and rehabilitation set. J Rehabil Med. (2016) 48:508–14. doi: 10.2340/16501977-2066
62. Reed GM, Lux JB, Bufka LF, Trask C, Peterson DB, Stark S, et al. Operationalizing the international classification of functioning, disability and health in clinical settings. Rehabil Psychol. (2005) 2005:122–31. doi: 10.1037/0090-5550.50.2.122
63. Tempest S, Harries P, Kilbride C, De Souza L. To adopt is to adapt: the process of implementing the ICF with an acute stroke multidisciplinary team in England. Disabil Rehabil. (2012) 34:1686–94. doi: 10.3109/09638288.2012.658489
64. Branch IR. The ICF Intervention Table. (2022). Available online at: https://www.icf-casestudies.org (accessed August 9, 2022).
65. Mehrholz J, Thomas S, Werner C, Kugler J, Pohl M, Elsner B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. (2017) 5:Cd006185. doi: 10.1002/14651858.CD006185.pub4
66. Su F, Xu W. Enhancing brain plasticity to promote stroke recovery. Front Neurol. (2020) 11:554089. doi: 10.3389/fneur.2020.554089
67. Epple C, Maurer-Burkhard B, Lichti M-C, Steiner T. Vojta therapy improves postural control in very early stroke rehabilitation: a randomised controlled pilot trial. Neurol Res Pract. (2020) 2:23. doi: 10.1186/s42466-020-00070-4
68. Gunning E, Uszynski MK. Effectiveness of the proprioceptive neuromuscular facilitation method on gait parameters in patients with stroke: a systematic review. Arch Phys Med Rehabil. (2019) 100:980–6. doi: 10.1016/j.apmr.2018.11.020
69. Rasova K, Prochazkova M, Tintera J, Ibrahim I, Zimova D, Stetkarova I. Motor programme activating therapy influences adaptive brain functions in multiple sclerosis: clinical and MRI study. Int J Rehabil Res. (2015) 38:49–54. doi: 10.1097/MRR.0000000000000090
70. Rasová K, Martinková P, Soler B, Freeman J, Cattaneo D, Jonsdottir J, et al. Real-world goal setting and use of outcome measures according to the international classification of functioning, disability and health: a european survey of physical therapy practice in multiple sclerosis. Int J Environ Res Public Health. (2020) 17:4774. doi: 10.3390/ijerph17134774
71. Haigh R, Tennant A, Biering-Sorensen F, Grimby G, Marincek C, Phillips S, et al. The use of outcome measures in physical medicine and rehabilitation within Europe. J Rehabil Med. (2001) 33:273–8. doi: 10.1080/165019701753236464
72. Havlík J, Horák P, Rasová K, Rezníčková J, Zeman J. The evaluation of the tremor: signal database of healthy control subjects. Praha: IFMBE Proceedings (2018).
73. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. (1971) 9:97–113. doi: 10.1016/0028-3932(71)90067-4
74. Costa PT, McCrae RR. Revised NEO Personality Inventory (NEO-PIR) and NEO Five Factor Inventory (NEO-FFI) Professional Manual. Odessa, FL: Psychological Assessment Resources (1992).
75. Wilson JT, Hareendran A, Grant M, Baird T, Schulz UG, Muir KW, et al. Improving the assessment of outcomes in stroke: use of a structured interview to assign grades on the modified rankin scale. Stroke. (2002) 33:2243–6. doi: 10.1161/01.STR.0000027437.22450.BD
76. Mediano MFF, Mok Y, Coresh J, Kucharska-Newton A, Palta P, Lakshminarayan K, et al. Prestroke physical activity and adverse health outcomes after stroke in the atherosclerosis risk in communities study. Stroke. (2021) 52:2086–95. doi: 10.1161/STROKEAHA.120.032695
77. Lyden P, Raman R, Liu L, Emr M, Warren M, Marler J. National institutes of health stroke scale certification is reliable across multiple venues. Stroke. (2009) 40:2507–11. doi: 10.1161/STROKEAHA.108.532069
78. Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet. (1991) 337:1521–6. doi: 10.1016/0140-6736(91)93206-O
79. Reeves M, Lisabeth L, Williams L, Katzan I, Kapral M, Deutsch A, et al. Patient-reported outcome measures (PROMs) for acute stroke: rationale, methods and future directions. Stroke. (2018) 49:1549–56. doi: 10.1161/STROKEAHA.117.018912
80. Hays RD, Bjorner JB, Revicki DA, Spritzer KL, Cella D. Development of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global items. Qual Life Res. (2009) 18:873–80. doi: 10.1007/s11136-009-9496-9
81. Ustun TB Kostanjesek N Chatterji S Rehm J World Health Organisation. Measuring health and disability: manual for WHO disability assessment schedule (WHODAS 2.0). In: Üstiün TB, Kostanjsek N, Chatterji S, Rehm J. Geneva: World Health Organization (2010). Available online at: https://apps.who.int/iris/handle/10665/43974
82. Ottenbacher KJ, Cusick A. Goal attainment scaling as a method of clinical service evaluation. Am J Occup Ther. (1990) 44:519–25. doi: 10.5014/ajot.44.6.519
83. Turner-Stokes L, Williams H, Johnson J. Goal attainment scaling: does it provide added value as a person-centred measure for evaluation of outcome in neurorehabilitation following acquired brain injury? J Rehabil Med. (2009) 41:528–35. doi: 10.2340/16501977-0383
84. Bertrand AM, Mercier C, Bourbonnais D, Desrosiers J, Gravel D. Reliability of maximal static strength measurements of the arms in subjects with hemiparesis. Clin Rehabil. (2007) 21:248–57. doi: 10.1177/0269215506070792
85. Chen HM, Chen CC, Hsueh IP, Huang SL, Hsieh CL. Test-retest reproducibility and smallest real difference of 5 hand function tests in patients with stroke. Neurorehabil Neural Repair. (2009) 23:435–40. doi: 10.1177/1545968308331146
86. Chen HF, Lin KC, Wu CY, Chen CL. Rasch validation and predictive validity of the action research arm test in patients receiving stroke rehabilitation. Arch Phys Med Rehabil. (2012) 93:1039–45. doi: 10.1016/j.apmr.2011.11.033
87. Uswatte G, Taub E, Morris D, Vignolo M, McCulloch K. Reliability and validity of the upper-extremity motor activity log-14 for measuring real-world arm use. Stroke. (2005) 36:2493–6. doi: 10.1161/01.STR.0000185928.90848.2e
88. Persson CU, Danielsson A, Sunnerhagen KS, Grimby-Ekman A, Hansson PO. Timed up & go as a measure for longitudinal change in mobility after stroke - postural stroke study in gothenburg (POSTGOT). J Neuroeng Rehabil. (2014) 11:83. doi: 10.1186/1743-0003-11-83
89. Blum L, Korner-Bitensky N. Usefulness of the berg balance scale in stroke rehabilitation: a systematic review. Phys Ther. (2008) 88:559–66. doi: 10.2522/ptj.20070205
90. Cheng DK, Nelson M, Brooks D, Salbach NM. Validation of stroke-specific protocols for the 10-meter walk test and 6-minute walk test conducted using 15-meter and 30-meter walkways. Top Stroke Rehabil. (2020) 27:251–61. doi: 10.1080/10749357.2019.1691815
91. Ring H, Feder M, Schwartz J, Samuels G. Functional measures of first-stroke rehabilitation inpatients: usefulness of the functional independence measure total score with a clinical rationale. Arch Phys Med Rehabil. (1997) 78:630–5. doi: 10.1016/S0003-9993(97)90429-9
92. Kostalova M, Mrackova M, Marecek R, Berankova D, Eliasova I, Janousova E, et al. The 3F test dysarthric profile—normative speach values in Czech. Cesk Slov Neurol Neurochir. (2013) 76:614–18.
93. Rusz J, Tykalova T, Ramig LO, Tripoliti E. Guidelines for speech recording and acoustic analyses in dysarthrias of movement disorders. Mov Disord. (2021) 36:803–14. doi: 10.1002/mds.28465
94. Nakase-Thompson R, Manning E, Sherer M, Yablon SA, Gontkovsky SL, Vickery C. Brief assessment of severe language impairments: initial validation of the mississippi aphasia screening test. Brain Injury. (2005) 19:685–91. doi: 10.1080/02699050400025331
96. Jaywant A, Toglia J, Gunning FM, O'Dell MW. Subgroups defined by the montreal cognitive assessment differ in functional gain during acute inpatient stroke rehabilitation. Arch Phys Med Rehabil. (2020) 101:220–6. doi: 10.1016/j.apmr.2019.08.474
97. Bartos A, Fayette D. Validation of the czech montreal cognitive assessment for mild cognitive impairment due to Alzheimer disease and czech norms in 1,552 elderly persons. Dement Geriatr Cogn Disord. (2018) 46:335–45. doi: 10.1159/000494489
98. Bartoš A. Two original Czech tests for memory evaluation in three minutes – amnesia light and brief assessment (ALBA) [article in Czech: Dvě pu°vodní české zkoušky k vyšetrení paměti za tři minuty - Amnesia Light and Brief Assessment (ALBA)]. Cesk Slov Neurol N. (2019) 82:420–9. doi: 10.14735/amcsnn2019420
99. Bartoš A, Diondet S. Amnesia light and brief assessment (ALBA) test – the second version and repeated examinations. [article in Czech: Test Amnesia Light and Brief Assessment (ALBA) – druhá verze a opakovaná vyšetrení]. Cesk Slov Neurol N. (2020) 83:535–43. doi: 10.14735/amcsnn2020535
100. Bartoš A. Do not test but POBAV (ENTERTAIN) – written intentional naming of pictures and their recall as a brief cognitive test [article in Czech: Netestuj, ale POBAV: písemné záměrné Pojmenování OBrázku A jejich Vybavení jako krátká kognitivní zkouška]. Cesk Slov Neurol N. (2016) 79:671–9. Available online at: https://www.csnn.eu/casopisy/ceska-slovenska-neurologie/2016-6-4/netestuj-ale-pobav-pisemne-zamerne-pojmenovani-obrazku-a-jejich-vybaveni-jako-kratka-kognitivni-zkouska-59479
101. Cella D, Lai JS, Nowinski CJ, Victorson D, Peterman A, Miller D, et al. Neuro-QOL: brief measures of health-related quality of life for clinical research in neurology. Neurology. (2012) 78:1860–7. doi: 10.1212/WNL.0b013e318258f744
102. Benjamini Y, Drai D, Elmer G, Kafkafi N, Golani I. Controlling the false discovery rate in behavior genetics research. Behav Brain Res. (2001) 125:279–84. doi: 10.1016/S0166-4328(01)00297-2
103. Team RC. A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2021).
104. Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. (2015) 67:1–48. doi: 10.18637/jss.v067.i01
105. Pinheiro JBD, DebRoy S, Sarkar D. R Core Team. _nlme: Linear Nonlinear Mixed Effects Models_. R package version 3.1-152. (2021). Available online at: https://CRAN.R-project.org/package=nlme> (accessed May 30, 2022).
106. Hladká A, Martinková P. difNLR: generalized logistic regression models for DIF and DDF detection. R J. (2020) 12:300–23. doi: 10.32614/RJ-2020-014
Keywords: ischemic stroke, lncRNA—long non-coding RNA, motor disability, rehabilitation, physiotherapy, motor recovery, international classification of functioning, disability and health model
Citation: Řasová K, Martinková P, Vařejková M, Miznerová B, Pavlíková M, Hlinovská J, Hlinovský D, Philippová Š, Novotný M, Pospíšilová K, Biedková P, Vojíková R, Havlík J, O'Leary VB, Černá M, Bartoš A and Philipp T (2022) COMIRESTROKE—A clinical study protocol for monitoring clinical effect and molecular biological readouts of COMprehensive Intensive REhabilitation program after STROKE: A four-arm parallel-group randomized double blinded controlled trial with a longitudinal design. Front. Neurol. 13:954712. doi: 10.3389/fneur.2022.954712
Received: 30 May 2022; Accepted: 17 October 2022;
Published: 01 November 2022.
Edited by:
Domenico Antonio Restivo, University of Messina, ItalyReviewed by:
Susanne Palmcrantz, Karolinska Institutet (KI), SwedenGelu Onose, University of Medicine and Pharmacy “Carol Davila”, Romania
Copyright © 2022 Řasová, Martinková, Vařejková, Miznerová, Pavlíková, Hlinovská, Hlinovský, Philippová, Novotný, Pospíšilová, Biedková, Vojíková, Havlík, O'Leary, Černá, Bartoš and Philipp. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patrícia Martinková, martinkova@cs.cas.cz; Tom Philipp, tom.philipp@ftn.cz; Kamila Řasová, kamila.rasova@gmail.com