
Combined Use of Presepsin and (1,3)-β-D-glucan as Biomarkers for Diagnosing Candida Sepsis and Monitoring the Effectiveness of Treatment in Critically Ill Patients

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Patient Selection, and Outcome
2.2. Samples and Laboratory
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics and Outcome
3.2. PSEP Exhibits the Highest Predictive Value for 28-Day Mortality
3.3. Serum CRP, PCT, PSEP, and BDG for Differentiation between Candida and Bacterial Sepsis
3.4. Monitoring of Successful Echinocandin Therapy
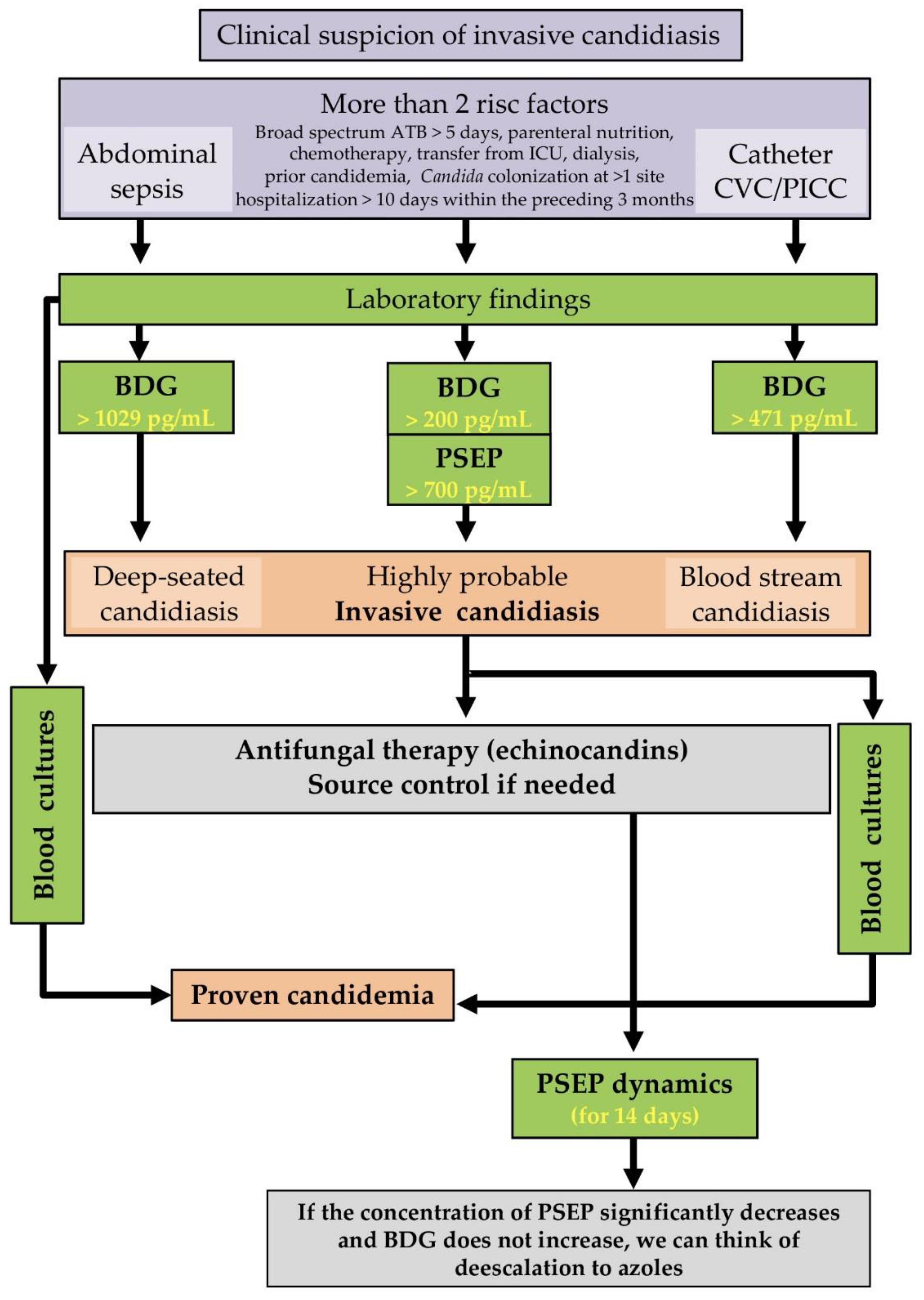
3.5. Proposal for the Use of Results in Clinical Practice
4. Discussion
4.1. PCT and PSEP in Sepsis and Sepsis-Related Mortality
4.2. PSEP and Renal Function
4.3. Predictive Value of Biomarker Combinations in Invasive Candidiasis
4.4. PSEP, Monitoring, and Prediction of Successful Treatment
4.5. Proposal for the Use of Results in Clinical Practice
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rüping, M.J.; Vehreschild, J.J.; Cornely, O.A. Patients at high risk of invasive fungal infections: When and how to treat. Drugs 2008, 68, 1941–1962. [Google Scholar] [CrossRef] [PubMed]
- Tóth, R.; Nosek, J.; Mora-Montes, H.M.; Gabaldon, T.; Bliss, J.M.; Nosanchuk, J.D.; Turner, S.A.; Butler, G.; Vágvölgyi, C.; Gácser, A. Candida parapsilosis: From Genes to the Bedside. Clin. Microbiol. Rev. 2019, 32, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacobbe, D.R.; Maraolo, A.E.; Simeon, V.; Magnè, F.; Pace, M.C.; Gentile, I.; Chiodini, P.; Viscoli, C.; Sanguinetti, M.; Mikulska, M.; et al. Changes in the relative prevalence of candidaemia due to non-albicans Candida species in adult in-patients: A systematic review, meta-analysis and meta-regression. Mycoses 2020, 63, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Vena, A.; Wolff, M. Diagnosis and Treatment of Candidemia in the Intensive Care Unit. Semin. Respir. Crit. Care Med. 2019, 40, 524–539. [Google Scholar] [CrossRef]
- Mellinghoff, S.C.; Cornely, O.A.; Jung, N. Essentials in Candida bloodstream infection. Infection 2018, 46, 897–899. [Google Scholar] [CrossRef] [PubMed]
- Bloos, F.; Held, J.; Schlattmann, P.; Brillinger, N.; Kurzai, O.; Cornely, O.A.; Thomas-Ruddel, D. (1,3)-beta-D-glucan-based diagnosis of invasive Candida infection versus culture-based diagnosis in patients with sepsis and with an increased risk of invasive Candida infection (CandiSep): Study protocol for a randomized controlled trial. Trials 2018, 19, 472. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Mikulska, M.; Tumbarello, M.; Furfaro, E.; Spadaro, M.; Losito, A.R.; Mesini, A.; De Pascale, G.; Marchese, A.; Bruzzone, M.; et al. Combined use of serum (1,3)-beta-D-glucan and procalcitonin for the early differential diagnosis between candidaemia and bacteraemia in intensive care units. Crit. Care 2017, 21, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, M.; Russo, A.; Righi, E.; Dolso, E.; Merelli, M.; D’Aurizio, F.; Sartor, A.; Curcio, F. Role of procalcitonin in predicting etiology in bacteremic patients: Report from a large single-center experience. J. Infect. Public Health 2019, 13, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Wen, M.Y.; Huang, L.Q.; Yang, F.; Ye, J.K.; Cai, G.X.; Li, X.S.; Ding, H.G.; Zeng, H.K. Presepsin level in predicting patients’ in-hospital mortality from sepsis under sepsis-3 criteria. Ther. Clin. Risk Manag. 2019, 15, 733–739. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, T.; Nishimura, T.; Kaga, S.; Uchida, K.; Tachibana, Y.; Esaki, M.; Fukushima, W.; Kondo, K.; Mizobata, Y. Diagnostic accuracy of presepsin for sepsis by the new Sepsis-3 definitions. Am. J. Emerg. Med. 2019, 37, 1936–1941. [Google Scholar] [CrossRef]
- Bamba, Y.; Moro, H.; Aoki, N.; Koizumi, T.; Ohshima, Y.; Watanabe, S.; Sakagami, T.; Koya, T.; Takada, T.; Kikuchi, T. Increased presepsin levels are associated with the severity of fungal bloodstream infections. PLoS ONE 2018, 13, e0206089. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Azoulay, E.; Kullberg, B.J.; Ruhnke, M.; Shoham, S.; Vazquez, J.; Giacobbe, D.R.; Calandra, T. EORTC/MSGERC Definitions of Invasive Fungal Diseases: Summary of Activities of the Intensive Care Unit Working Group. Clin. Infect. Dis. 2021, 72, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.; Suter, P.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure; Springer: Berlin/Heidelberg, Germany, 1996. [Google Scholar]
- Vincent, J.; De Mendonça, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.; Sprung, C.; Colardyn, F.; Blecher, S. Working Group on “Sepsis-Related Problems” of the European Society of Intensive Care Medicine. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Marazzi, A.; Freeman, J.; Chioléro, R. Evaluation of the consistency of Acute Physiology and Chronic Health Evaluation (APACHE II) scoring in a surgical intensive care unit. Crit. Care Med. 1992, 20, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Baden, L.R.; Marty, F.M. Post-diagnostic kinetics of the (1→3)-beta-D-glucan assay in invasive aspergillosis, invasive candidiasis and Pneumocystis jirovecii pneumonia. Clin. Microbiol. Infect. 2012, 18, E122–E127. [Google Scholar] [CrossRef] [Green Version]
- Charles, P.E.; Tinel, C.; Barbar, S.; Aho, S.; Prin, S.; Doise, J.M.; Olsson, N.O.; Blettery, B.; Quenot, J.P. Procalcitonin kinetics within the first days of sepsis: Relationship with the appropriateness of antibiotic therapy and the outcome. Crit. Care 2009, 13, R38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, Y.; Hoshino, K.; Kiyomi, F.; Kawano, Y.; Mizunuma, M.; Tanaka, J.; Nishida, T.; Ishikura, H. Comparison of accuracy of presepsin and procalcitonin concentrations in diagnosing sepsis in patients with and without acute kidney injury. Clin. Chim. Acta Int. J. Clin. Chem. 2019, 490, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Umemura, Y.; Hayashida, K.; Hara, Y.; Aihara, M.; Yamakawa, K. Diagnostic value of procalcitonin and presepsin for sepsis in critically ill adult patients: A systematic review and meta-analysis. J. Intensive Care 2019, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Cortegiani, A.; Misseri, G.; Ippolito, M.; Bassetti, M.; Giarratano, A.; Martin-Loeches, I.; Einav, S. Procalcitonin levels in candidemia versus bacteremia: A systematic review. Crit. Care 2019, 23, 190. [Google Scholar] [CrossRef] [Green Version]
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Nakamura, Y.; Ishikura, H.; Nishida, T.; Kawano, Y.; Yuge, R.; Ichiki, R.; Murai, A. Usefulness of presepsin in the diagnosis of sepsis in patients with or without acute kidney injury. BMC Anesthesiol. 2014, 14, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyoshi, M.; Inoue, Y.; Nishioka, M.; Ikegame, A.; Nakao, T.; Kishi, S.; Doi, T.; Nagai, K. Clinical evaluation of presepsin considering renal function. PLoS ONE 2019, 14, e0215791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, G.; Shibata, S.; Fukui, Y.; Okamura, Y.; Inoue, Y. Diagnostic accuracy of procalcitonin and presepsin for infectious disease in patients with acute kidney injury. Diagn. Microbiol. Infect. Dis. 2016, 86, 205–210. [Google Scholar] [CrossRef]
- Takahashi, G.; Shibata, S.; Ishikura, H.; Miura, M.; Fukui, Y.; Inoue, Y.; Endo, S. Presepsin in the prognosis of infectious diseases and diagnosis of infectious disseminated intravascular coagulation: A prospective, multicentre, observational study. Eur. J. Anaesthesiol. 2015, 32, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Velissaris, D.; Zareifopoulos, N.; Karamouzos, V.; Karanikolas, E.; Pierrakos, C.; Koniari, I.; Karanikolas, M. Presepsin as a Diagnostic and Prognostic Biomarker in Sepsis. Cureus 2021, 13, e15019. [Google Scholar] [CrossRef] [PubMed]
- Nagata, T.; Yasuda, Y.; Ando, M.; Abe, T.; Katsuno, T.; Kato, S.; Tsuboi, N.; Matsuo, S.; Maruyama, S. Clinical impact of kidney function on presepsin levels. PLoS ONE 2015, 10, e0129159. [Google Scholar] [CrossRef] [Green Version]
- Shiota, J. Changes of Early Sepsis Biomarker Presepsin Level during Hemodialysis: Influence of beta2-Microglobulin Clearance of Dialysis Membrane: A Preliminary Study. Kidney Dis. 2019, 5, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Scudeller, L.; Bassetti, M.; Concia, E.; Corrao, S.; Cristini, F.; De Rosa, F.G.; Del Bono, V.; Durante-Mangoni, E.; Falcone, M.; Menichetti, F.; et al. MEDical wards Invasive Candidiasis ALgorithms (MEDICAL):Consensus proposal for management. Eur. J. Int. Med. 2016, 34, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Martin-Loeches, I.; Antonelli, M.; Cuenca-Estrella, M.; Dimopoulos, G.; Einav, S.; De Waele, J.J.; Garnacho-Montero, J.; Kanj, S.S.; Machado, F.R.; Montravers, P.; et al. ESICM/ESCMID task force on practical management of invasive candidiasis in critically ill patients. Intensive Care Med. 2019, 45, 789–805. [Google Scholar] [CrossRef]
- White, P.L.; Posso, R.; Parr, C.; Price, J.S.; Finkelman, M.; Barnes, R.A. The presence of (1-3)-β-D-Glucan as prognostic marker in patients post major abdominal surgery. Clin. Infect. Dis. 2020, 73, e1415–e1422. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Chen, J.; Cai, B.; Zhang, J.; Li, L.; Liu, C.; Kang, Y.; Wang, L. The use of PCT, CRP, IL-6 and SAA in critically ill patients for an early distinction between candidemia and Gram positive/negative bacteremia. J. Infect. 2012, 64, 438–440. [Google Scholar] [CrossRef] [PubMed]
- Sager, R.; Kutz, A.; Mueller, B.; Schuetz, P. Procalcitonin-guided diagnosis and antibiotic stewardship revisited. BMC Med. 2017, 15, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covington, E.W.; Roberts, M.Z.; Dong, J. Procalcitonin Monitoring as a Guide for Antimicrobial Therapy: A Review of Current Literature. Pharmacotherapy 2018, 38, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Beishuizen, A.; Broyles, M.; Ferrer, R.; Gavazzi, G.; Gluck, E.H.; González Del Castillo, J.; Jensen, J.U.; Kanizsai, P.L.; Kwa, A.L.H.; et al. Procalcitonin (PCT)-guided antibiotic stewardship: An international experts consensus on optimized clinical use. Clin. Chem. Lab. Med. 2019, 57, 1308–1318. [Google Scholar] [CrossRef] [PubMed]
- De Pascale, G.; Posteraro, B.; D’Arrigo, S.; Spinazzola, G.; Gaspari, R.; Bello, G.; Montini, L.M.; Cutuli, S.L.; Grieco, D.L.; Di Gravio, V.; et al. (1,3)-β-D-Glucan-based empirical antifungal interruption in suspected invasive candidiasis: A randomized trial. Crit. Care 2020, 24, 550. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, R.A.; Einav, S.; Leone, M.; Madách, K.; Martin, C.; Martin-Loeches, I. Management of invasive candidiasis and candidaemia in critically ill adults: Expert opinion of the European Society of Anaesthesia Intensive Care Scientific Subcommittee. J. Hosp. Infect. 2018, 98, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Dobias, R.; Jaworska, P.; Tomaskova, H.; Kanova, M.; Lyskova, P.; Vrba, Z.; Holub, C.; Svobodova, L.; Hamal, P.; Raska, M. Diagnostic value of serum galactomannan, (1-3)-beta-D-glucan, and Aspergillus fumigatus-specific IgA and IgG assays for invasive pulmonary aspergillosis in non-neutropenic patients. Mycoses 2018, 61, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, R.; Rappold, E.; Bogdan, C.; Held, J. Comparative Analysis of the Wako beta-Glucan Test and the Fungitell Assay for Diagnosis of Candidemia and Pneumocystis jirovecii Pneumonia. J. Clin. Microbiol. 2018, 56, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kritikos, A.; Poissy, J.; Croxatto, A.; Bochud, P.Y.; Pagani, J.L.; Lamoth, F. Impact of the Beta-Glucan Test on Management of Intensive Care Unit Patients at Risk for Invasive Candidiasis. J. Clin. Microbiol. 2020, 58, 19. [Google Scholar] [CrossRef] [PubMed]
- Zanoni, I.; Granucci, F. Role of CD14 in host protection against infections and in metabolism regulation. Front. Cell. Infect. Microbiol. 2013, 3, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shozushima, T.; Takahashi, G.; Matsumoto, N.; Kojika, M.; Okamura, Y.; Endo, S. Usefulness of presepsin (sCD14-ST) measurements as a marker for the diagnosis and severity of sepsis that satisfied diagnostic criteria of systemic inflammatory response syndrome. J. Infect. Chemother. 2011, 17, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Rogic, D.; Juros, G.F.; Petrik, J.; Vrancic, A.L. Advances and Pitfalls in Using Laboratory Biomarkers for the Diagnosis and Management of Sepsis. EJIFCC 2017, 28, 114–121. [Google Scholar] [PubMed]
- Chenevier-Gobeaux, C.; Bardet, V.; Poupet, H.; Poyart, C.; Borderie, D.; Claessens, Y.E. Presepsin (sCD14-ST) secretion and kinetics by peripheral blood mononuclear cells and monocytic THP-1 cell line. Ann. Biol. Clin. 2016, 74, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Endo, S.; Suzuki, Y.; Takahashi, G.; Shozushima, T.; Ishikura, H.; Murai, A.; Nishida, T.; Irie, Y.; Miura, M.; Iguchi, H.; et al. Usefulness of presepsin in the diagnosis of sepsis in a multicenter prospective study. J. Infect. Chemother. 2012, 18, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Carpio, R.; Zapata, J.; Spanuth, E.; Hess, G. Utility of presepsin (sCD14-ST) as a diagnostic and prognostic marker of sepsis in the emergency department. Clin. Chim. Acta 2015, 450, 169–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouadma, L.; Luyt, C.E.; Tubach, F.; Cracco, C.; Alvarez, A.; Schwebel, C.; Schortgen, F.; Lasocki, S.; Veber, B.; Dehoux, M.; et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): A multicentre randomised controlled trial. Lancet 2010, 375, 463–474. [Google Scholar] [CrossRef]
- Giavarina, D.; Carta, M. Determination of reference interval for presepsin, an early marker for sepsis. Biochem. Med. 2015, 25, 64–68. [Google Scholar] [CrossRef]
- Behnes, M.; Bertsch, T.; Lepiorz, D.; Lang, S.; Trinkmann, F.; Brueckmann, M.; Borggrefe, M.; Hoffmann, U. Diagnostic and prognostic utility of soluble CD 14 subtype (presepsin) for severe sepsis and septic shock during the first week of intensive care treatment. Crit. Care 2014, 18, 507. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Chen, Y.X.; Yin, Q.; Zhao, Y.Z.; Li, C.S. Diagnostic value and prognostic evaluation of Presepsin for sepsis in an emergency department. Crit. Care 2013, 17, R244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Guadiana Romualdo, L.G.; Torrella, P.E.; Acebes, S.R.; Oton, M.D.; Sanchez, R.J.; Holgado, A.H.; Santos, E.J.; Freire, A.O. Diagnostic accuracy of presepsin (sCD14-ST) as a biomarker of infection and sepsis in the emergency department. Clin. Chim. Acta 2017, 464, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Pugni, L.; Pietrasanta, C.; Milani, S.; Vener, C.; Ronchi, A.; Falbo, M.; Arghittu, M.; Mosca, F. Presepsin (Soluble CD14 Subtype): Reference Ranges of a New Sepsis Marker in Term and Preterm Neonates. PLoS ONE 2015, 10, e0146020. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | Candidemia * (n = 58; 35%) | Bacteremia ** (n = 107; 65%) | p-Value |
|---|---|---|---|
| Demographic | |||
| Median age (IQR) | 54 (46–72) | 60 (46–72) | 0.668 † |
| Male gender | 34 (58%) | 76 (71%) | 0.116 ✕ |
| Mortality rate | 19 (33%) | 24 (22%) | 0.141 ♢ |
| Clinical type of patients | n (%) | n (%) | |
| Surgical | 19 (33%) | 25 (23%) | 0.193 † |
| Traumatic | 2 (3%) | 6 (6%) | 0.714 ♢ |
| Medical | 37 (64%) | 76 (71%) | 0.340 † |
| Previous abdominal surgery | 14 (24%) | 13 (12%) | 0.047 † |
| Diabetes mellitus | 1 (2%) | 0 (0%) | 0.352 ♢ |
| Inserted CVC or PICC | 58 (100%) | 74 (69%) | <0.001 † |
| Chronic renal disease | 12 (21%) | 12 (11%) | 0.099 † |
| Corticosteroid therapy | 10 (17%) | 14 (13%) | 0.470 † |
| Preceding antibiotic therapy | 48 (83%) | 45 (42%) | <0.001 † |
| Preceding antifungal therapy | 6 (10%) | 7 (6.5%) | 0.387 † |
| Prescoring | median (IQR) | median (IQR) | |
| SOFA | 3.5 (2–9) | 6.0 (2–8) | 0.191 ✕ |
| APACHE II | 12.5 (8–18) | 15.0 (10–21) | 0.200 ✕ |
| Time from admission to candidemia or bacteremia, days | 23.0 (18–30) | 13 (10–18) | <0.001 ✕ |
| Acute kidney injury stage (serum creatinine range) | n = 18 (31%) | n = 40 (33%) | |
| Stage 1 (110–170 µmol/L) | 4 (22%) | 16 (40%) | |
| Stage 2 (171–299 µmol/L) | 11 (61%) | 17 (43%) | 0.362 † |
| Stage 3 (300 ≥ 440 µmol/L) | 3 (17%) | 7 (17%) | |
| Median serum creatinine, µmol/L (IQR) | 274 (178–348) | 180 (141–321) | 0.217 ✕ |
| CRRT | 3 (5%) | 3 (3%) | |
| RRT | 10 (17%) | 12 (11%) |
| Assessed Biomarkers (Recent Cut-Off) | Candidemia n (%) | Bacteremia n (%) | p-Value |
|---|---|---|---|
| CRP (≥5 mg/mL) | 58 (100%) | 107 (100%) | 0.999 † |
| CRP (≥130 mg/mL) | 22 (38%) | 73 (68%) | <0.001 † |
| PCT (>0.5 ng/l) | 52 (90%) | 91 (85%) | 0.406 † |
| PCT (<3 ng/l) * | 44 (76%) | 60 (56%) | 0.012 † |
| PSEP (>350 pg/mL) | 58 (100%) | 107 (100%) | 0.999 ✕ |
| PSEP (>700 pg/mL) ** | 58 (100%) | 101 (94%) | 0.091 ✕ |
| BDG (≥80 pg/mL) | 58 (100%) | 19 (18%) | <0.001 ✕ |
| BDG (≥200 pg/mL) | 56 (97%) | 3 (3%) | <0.001 † |
| Median Values (Conc.) | Candidemia (IQR) | Bacteremia (IQR) | p-Value |
| CRP (mg/L) | 104 (78–150) | 164 (101–234) | <0.001 ♢ |
| PCT (ng/L) | 1.6 (0.90–2.80) | 2.4 (1.03–8.54) | 0.105 ♢ |
| PSEP (pg/mL) | 1784 (1203–3259) | 1963 (1313–3524) | 0.777 ♢ |
| BDG (pg/mL) | 1029 (500–1176) | 35 (0–73) | <0.001 ♢ |
| CRP 130 mg/mL | PCT 0.5 ng/L | PCT 0–3 ng/L | PSEP >700 pg/mL | BDG ≥200 pg/mL | BDG/PSE * | |
|---|---|---|---|---|---|---|
| Sensitivity (%) | 37.9 | 89.7 | 75.9 | 100 | 96.6 | 94.8 |
| 95% CI | 25.5–51.6 | 78.8–96.1 | 62.8–86.1 | 93.8–100 | 88.1–99.6 | 85.6–98.9 |
| Specificity (%) | 31.8 | 15.0 | 43.9 | 5.6 | 97.2 | 100 |
| 95% CI | 23.1–41.5 | 8.8–23.1 | 34.3–53.9 | 2.1–11.8 | 92.0–99.4 | 96.6–100 |
| PPV (%) | 23.2 | 36.4 | 42.3 | 36.5 | 94.9 | 100.0 |
| 95% CI | 15.1–32.9 | 28.5–44.8 | 32.7–52.4 | 29.0–44.5 | 85.9–98.9 | 93.5–100.0 |
| NPV (%) | 48.6 | 72.7 | 77.0 | 100 | 98.1 | 97.3 |
| 95% CI | 36.4–60.8 | 49.8–89.3 | 64.5–86.8 | 54.1–100 | 93.4–99.8 | 92.2–99.4 |
| AUC | 0.35 | 0.52 | 0.60 | 0.53 | 0.97 | 0.97 |
| 95% CI | 0.27–0.43 | 0.47–0.58 | 0.53–0.67 | 0.51–0.55 | 0.94–1.00 | 0.95–1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobiáš, R.; Káňová, M.; Petejová, N.; Pisti, Š.K.; Bocek, R.; Krejčí, E.; Stružková, H.; Cachová, M.; Tomášková, H.; Hamal, P.; et al. Combined Use of Presepsin and (1,3)-β-D-glucan as Biomarkers for Diagnosing Candida Sepsis and Monitoring the Effectiveness of Treatment in Critically Ill Patients. J. Fungi 2022, 8, 308. https://doi.org/10.3390/jof8030308
Dobiáš R, Káňová M, Petejová N, Pisti ŠK, Bocek R, Krejčí E, Stružková H, Cachová M, Tomášková H, Hamal P, et al. Combined Use of Presepsin and (1,3)-β-D-glucan as Biomarkers for Diagnosing Candida Sepsis and Monitoring the Effectiveness of Treatment in Critically Ill Patients. Journal of Fungi. 2022; 8(3):308. https://doi.org/10.3390/jof8030308
Chicago/Turabian StyleDobiáš, Radim, Marcela Káňová, Naděžda Petejová, Štefan Kis Pisti, Robert Bocek, Eva Krejčí, Helena Stružková, Michaela Cachová, Hana Tomášková, Petr Hamal, and et al. 2022. "Combined Use of Presepsin and (1,3)-β-D-glucan as Biomarkers for Diagnosing Candida Sepsis and Monitoring the Effectiveness of Treatment in Critically Ill Patients" Journal of Fungi 8, no. 3: 308. https://doi.org/10.3390/jof8030308