
Subretinal Implantation of Human Primary RPE Cells Cultured on Nanofibrous Membranes in Minipigs

 , , , , , , , , add
Show full author list
, , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Isolation and Cultivation of hRPEs
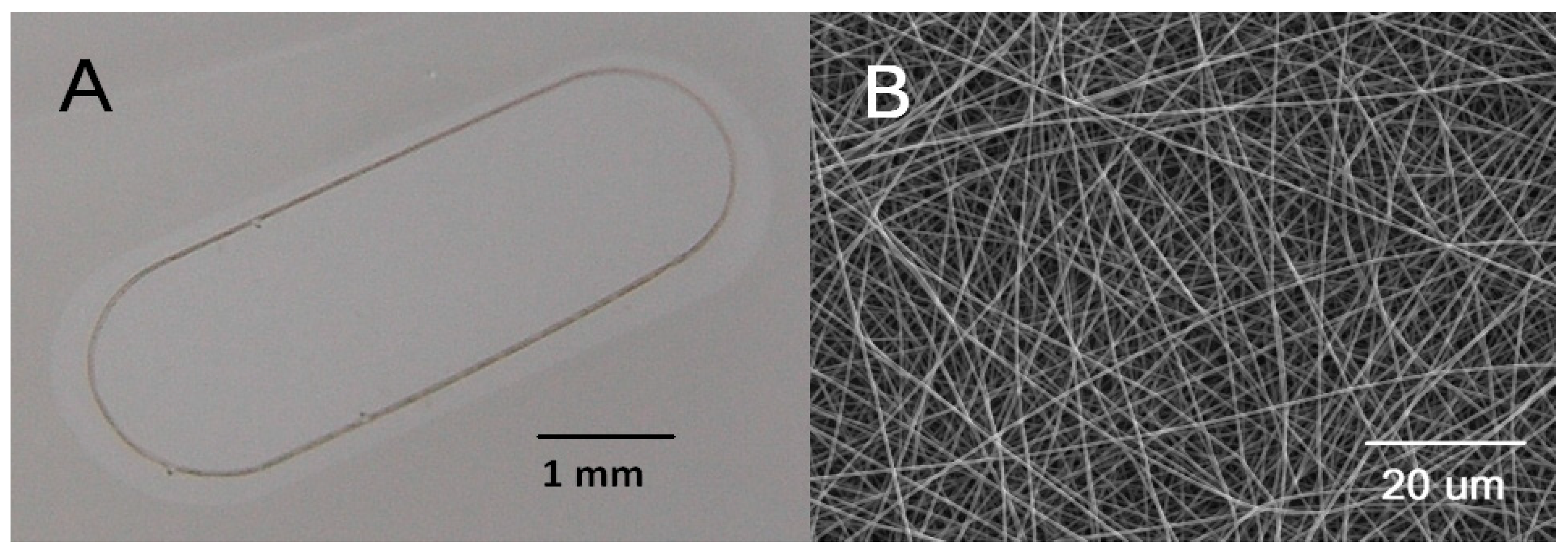
2.3. Ultrathin Nanofibrous Carrier for RPE Transplantation
2.4. Trans-Epithelial Electrical Resistance (TEER)
2.5. Implantation Injector
2.6. Animals Used for the Experimental Study
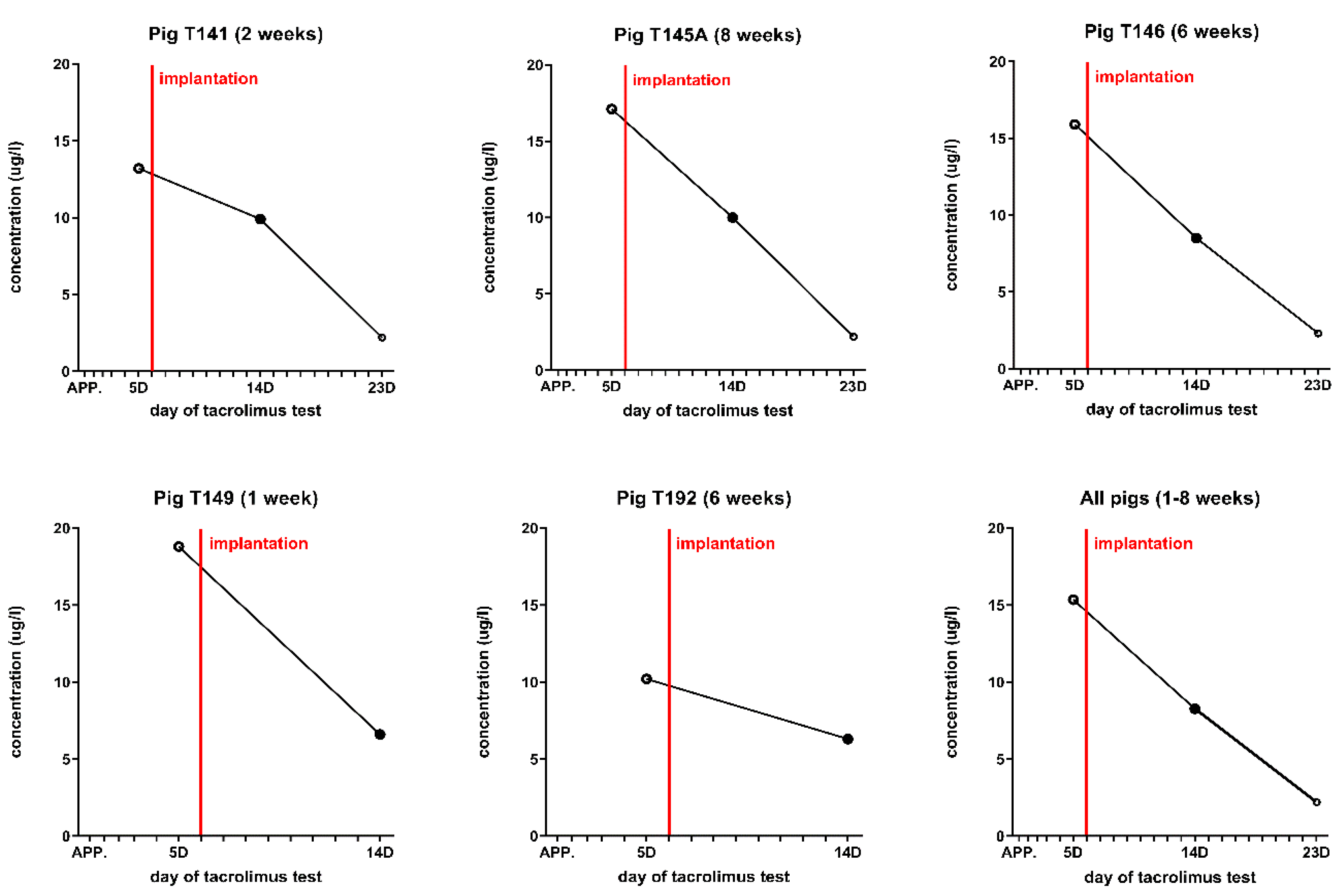
2.7. Immunosuppression of Minipigs
2.8. Implantation of hRPEs on a Nanofibrous Carrier into Minipigs
2.9. Surgical Technique
2.10. In Vivo Optical Coherence Tomography
2.11. Euthanasia and Tissue Processing
2.12. Immunohistochemical Analysis
2.13. Laser Scanning Confocal Microscopy
3. Results
3.1. Production of a Monolayer of hRPEs on a Nanofibrous Carrier
3.2. Trans-Epithelial Electrical Resistance (TEER)
3.3. Implantation of the hRPEs
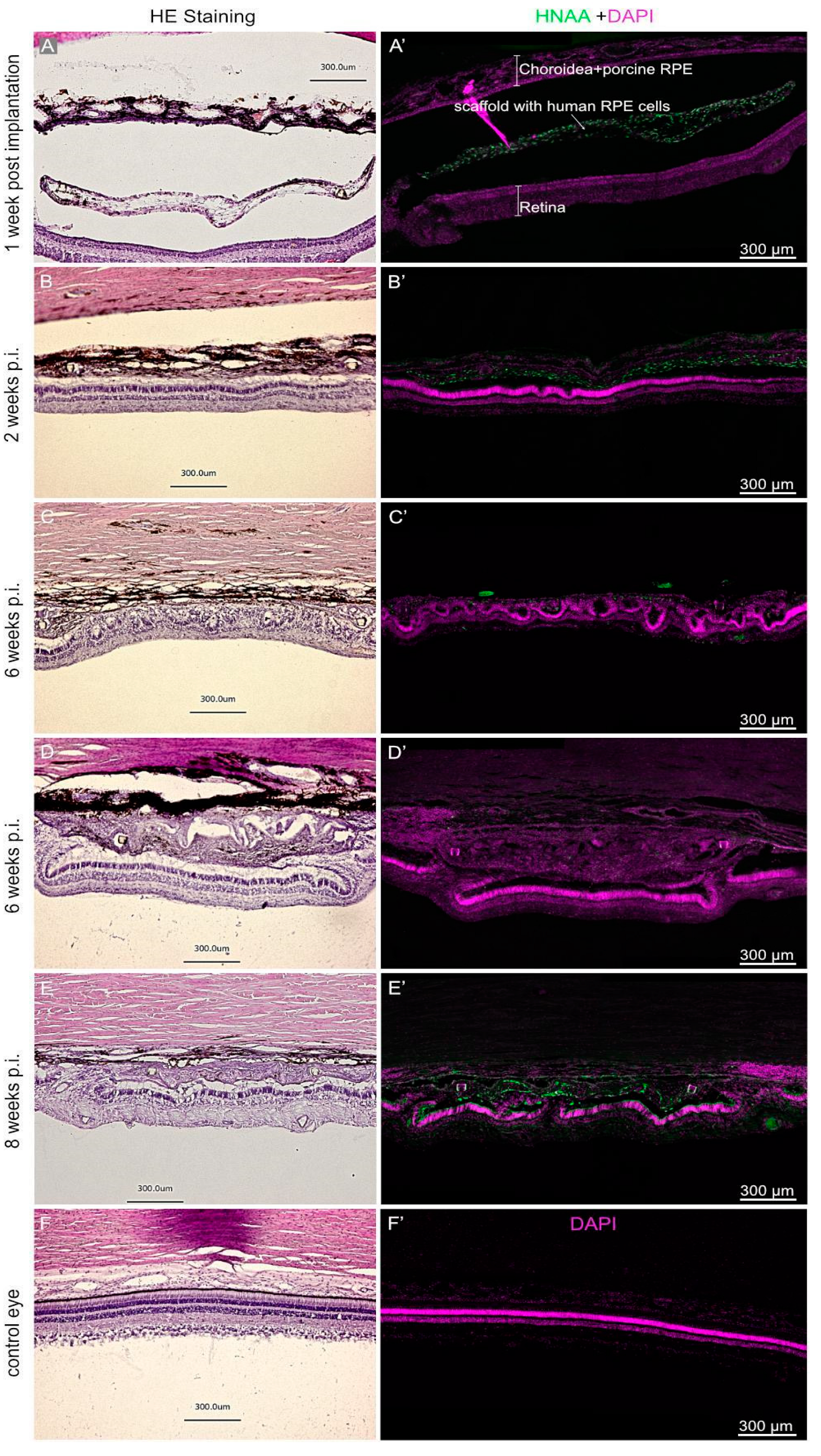
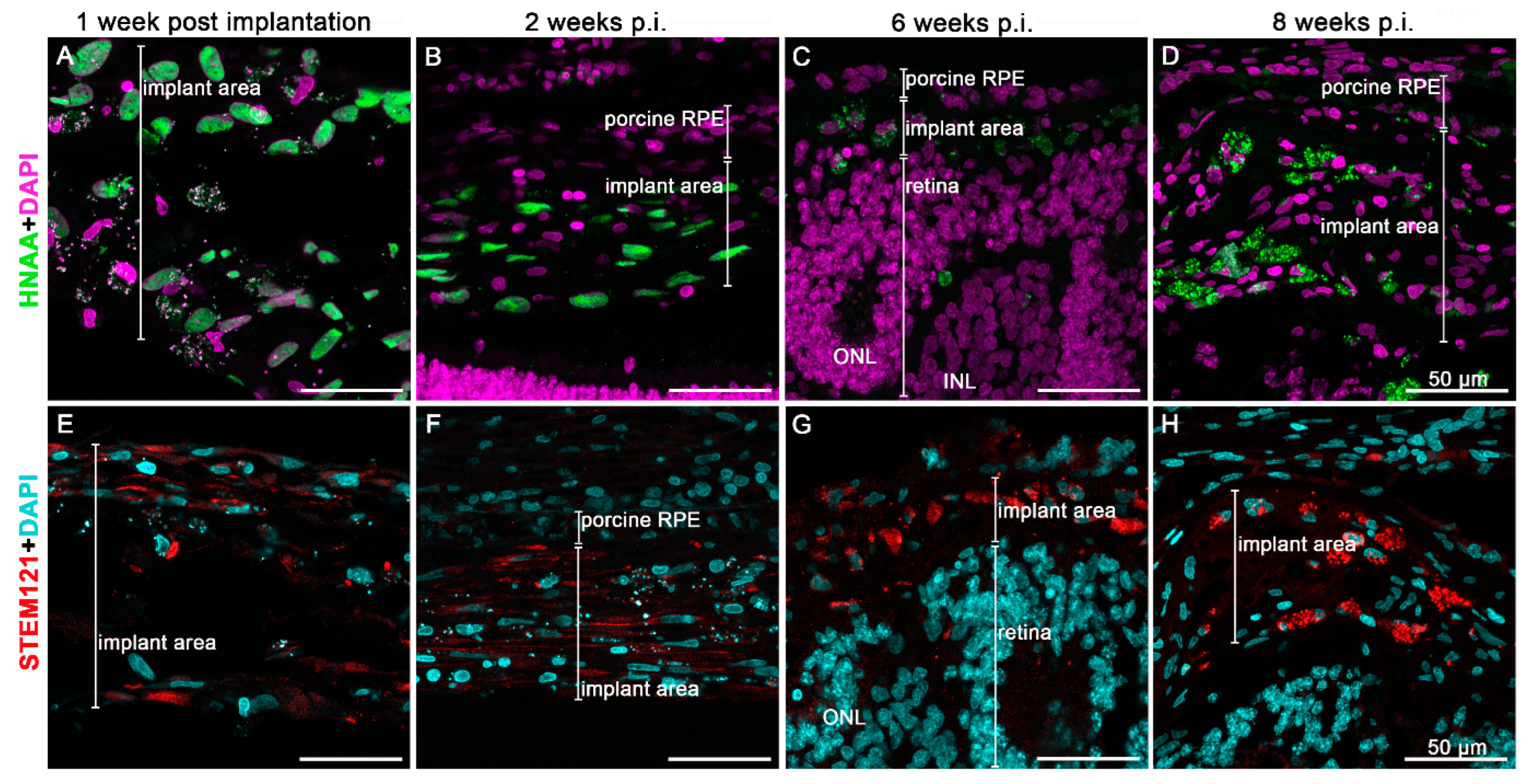
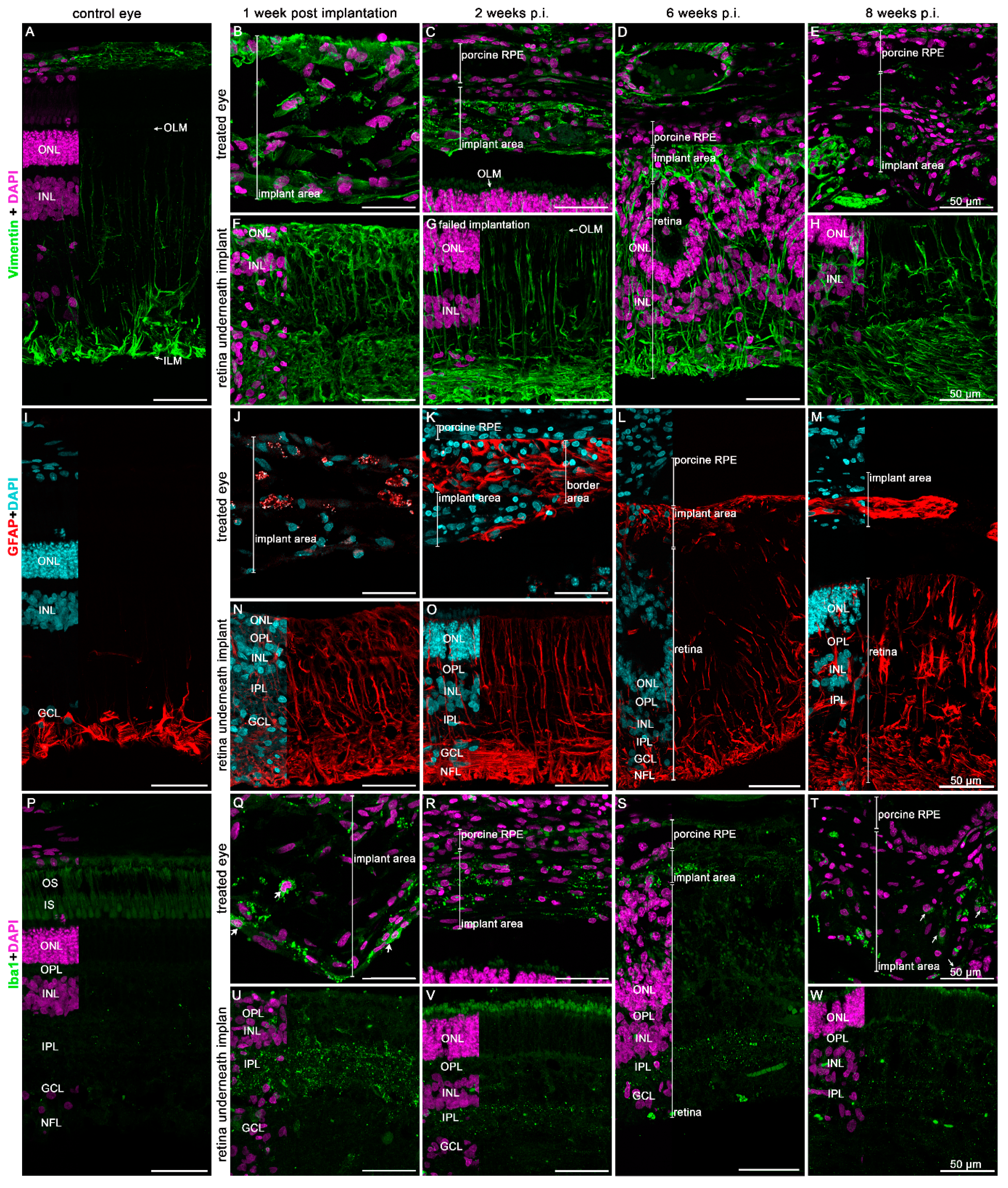
3.4. Immunohistochemical Analysis of the Implanted hRPEs
4. Discussion
4.1. RPE Preparation for Transplantation and Post-Implantation Characterization
4.2. RPE Surgical Transplantation
4.3. Injection of RPE Cell Monolayer
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jager, R.D.; Mieler, W.F.; Miller, J.W. Age-related macular degeneration. N. Engl. J. Med. 2008, 358, 2606–2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cachafeiro, M.; Bemelmans, A.P.; Samardzija, M.; Afanasieva, T.; Pournaras, J.-A.; Grimm, C.; Kostic, C.; Philippe, S.; Wenzel, A.; Arsenijevic, Y. Hyperactivation of retina by light in mice leads to photoreceptor cell death mediated by VEGF and retinal pigment epithelium permeability. Cell Death Dis. 2013, 4, e781. [Google Scholar] [CrossRef] [PubMed]
- Szatmari-Toth, M.; Kristof, E.; Vereb, Z.; Akhtar, S.; Facsko, A.; Fesus, L.; Kauppinen, A.; Kaarniranta, K.; Petrovski, G. Clearance of autophagy-associated dying retinal pigment epithelial cells—A possible source for inflammation in age-related macular degeneration. Cell Death Dis. 2016, 7, e2367. [Google Scholar] [CrossRef] [PubMed]
- Rivas, D.E.; Borot, A.; Cardenas, D.E.; Marcus, G.; Gu, X.; Herrmann, D.; Xu, J.; Tan, J.; Kormin, D.; Ma, G.; et al. Next Generation Driver for Attosecond and Laser-plasma Physics. Sci. Rep. 2017, 7, 5224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagymihaly, R.N.Y.; Ardan, T.; Motlik, J.; Eidet, J.R.; Moe, M.C.; Bergersen, L.H.; Lytvynchuk, L.; Petrovski, G. The retinal pigment epithelium: At the forefront of the blood-retinal barrier in physiology and disease. In Tissue Barriers in Disease, Injury and Regeneration; Elsevier: Amsterdam, The Netherlands, 2021; pp. 115–146. [Google Scholar]
- Fuhrmann, S.; Zou, C.; Levine, E.M. Retinal pigment epithelium development, plasticity, and tissue homeostasis. Exp. Eye Res. 2014, 123, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Sharma, R.; Bose, D.; Maminishkis, A.; Bharti, K. Retinal Pigment Epithelium Replacement Therapy for Age-Related Macular Degeneration: Are We There Yet? Annu. Rev. Pharmacol. Toxicol. 2020, 60, 553–572. [Google Scholar] [CrossRef]
- Holz, F.G.; Schmitz-Valckenberg, S.; Fleckenstein, M. Recent developments in the treatment of age-related macular degeneration. J. Clin. Investig. 2014, 124, 1430–1438. [Google Scholar] [CrossRef] [Green Version]
- Ammar, M.J.; Hsu, J.; Chiang, A.; Ho, A.C.; Regillo, C.D. Age-related macular degeneration therapy: A review. Curr. Opin. Ophthalmol. 2020, 31, 215–221. [Google Scholar] [CrossRef]
- Baradaran-Rafii, A.; Sarvari, M.; Alavi-Moghadam, S.; Payab, M.; Goodarzi, P.; Aghayan, H.R.; Larijani, B.; Rezaei-Tavirani, M.; Biglar, M.; Arjmand, B. Cell-based approaches towards treating age-related macular degeneration. Cell Tissue Bank. 2020, 21, 339–347. [Google Scholar] [CrossRef]
- Fernández-Robredo, P.; Sancho, A.; Johnen, S.; Recalde, S.; Gama, N.; Thumann, G.; Groll, J.; García-Layana, A. Current treatment limitations in age-related macular degeneration and future approaches based on cell therapy and tissue engineering. J. Ophthalmol. 2014, 2014, 510285. [Google Scholar] [CrossRef] [Green Version]
- Forest, D.L.; Johnson, L.V.; Clegg, D.O. Cellular models and therapies for age-related macular degeneration. Dis. Models Mech. 2015, 8, 421–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarbin, M.; Sugino, I.; Townes-Anderson, E. Concise Review: Update on Retinal Pigment Epithelium Transplantation for Age-Related Macular Degeneration. Stem Cells Transl. Med. 2019, 8, 466–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, R.; Khristov, V.; Rising, A.; Jha, B.S.; Dejene, R.; Hotaling, N.; Li, Y.; Stoddard, J.; Stankewicz, C.; Wan, Q.; et al. Clinical-grade stem cell-derived retinal pigment epithelium patch rescues retinal degeneration in rodents and pigs. Sci. Transl. Med. 2019, 11, eaat5580. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, P.; Booth, H.; Gutteridge, A.; Surmacz, B.; Louca, I.; Steer, J.; Kerby, J.; Whiting, P.J. Directing Differentiation of Pluripotent Stem Cells Toward Retinal Pigment Epithelium Lineage. Stem Cells Transl. Med. 2017, 6, 490–501. [Google Scholar] [CrossRef] [Green Version]
- Kuroda, T.; Ando, S.; Takeno, Y.; Kishino, A.; Kimura, T. Robust induction of retinal pigment epithelium cells from human induced pluripotent stem cells by inhibiting FGF/MAPK signaling. Stem Cell Res. 2019, 39, 101514. [Google Scholar] [CrossRef]
- Popelka, Š.; Studenovská, H.; Abelová, L.; Ardan, T.; Studený, P.; Straňák, Z.; Klíma, J.; Dvořánková, B.; Kotek, J.; Hodan, J.; et al. A frame-supported ultrathin electrospun polymer membrane for transplantation of retinal pigment epithelial cells. Biomed. Mater. 2015, 10, 045022. [Google Scholar] [CrossRef]
- Eichhorn, S.J.; Sampson, W.W. Statistical geometry of pores and statistics of porous nanofibrous assemblies. J. R. Soc. Interface 2005, 2, 309–318. [Google Scholar] [CrossRef]
- Vodicka, P.; Smetana, K., Jr.; Dvorankova, B.; Emerick, T.; Xu, Y.Z.; Ourednik, J.; Ourednik, V.; MotlÍk, J.A. The miniature pig as an animal model in biomedical research. Ann. N. Y. Acad. Sci. 2005, 1049, 161–171. [Google Scholar] [CrossRef]
- Sevc, J.; Goldberg, D.; van Gorp, S.; Leerink, M.; Juhas, S.; Juhasova, J.; Marsala, S.; Hruska-Plochan, M.; Hefferan, M.P.; Motlik, J.; et al. Effective long-term immunosuppression in rats by subcutaneously implanted sustained-release tacrolimus pellet: Effect on spinally grafted human neural precursor survival. Exp. Neurol. 2013, 248, 85–99. [Google Scholar] [CrossRef]
- Jin, Z.B.; Gao, M.L.; Deng, W.L.; Wu, K.C.; Sugita, S.; Mandai, M.; Takahashi, M. Stemming retinal regeneration with pluripotent stem cells. Prog. Retin. Eye Res. 2019, 69, 38–56. [Google Scholar] [CrossRef]
- O’Neill, H.C.; Limnios, I.J.; Barnett, N.L. Advancing a Stem Cell Therapy for Age-Related Macular Degeneration. Curr. Stem Cell Res. Ther. 2020, 15, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Bilic, J.; Izpisua Belmonte, J.C. Concise review: Induced pluripotent stem cells versus embryonic stem cells: Close enough or yet too far apart? Stem Cells 2012, 30, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Cabral de Guimaraes, T.A.; Daich Varela, M.; Georgiou, M.; Michaelides, M. Treatments for dry age-related macular degeneration: Therapeutic avenues, clinical trials and future directions. Br. J. Ophthalmol. 2021, 106, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Joussen, A.M.; Joeres, S.; Fawzy, N.; Heussen, F.M.; Llacer, H.; van Meurs, J.C.; Kirchhof, B. Autologous translocation of the choroid and retinal pigment epithelium in patients with geographic atrophy. Ophthalmology 2007, 114, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Da Cruz, L.; Fynes, K.; Georgiadis, O.; Kerby, J.; Luo, Y.H.; Ahmado, A.; Vernon, A.; Daniels, J.T.; Nommiste, B.; Hasan, S.M.; et al. Phase 1 clinical study of an embryonic stem cell-derived retinal pigment epithelium patch in age-related macular degeneration. Nat. Biotechnol. 2018, 36, 328–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bharti, K. Induced to cure: Engineering iPS cell derived RPE scaffolds to treat degenerative eye diseases. Acta Ophthalmol. 2015, 93. [Google Scholar] [CrossRef]
- Lee, D.Y.; Lorach, H.; Huie, P.; Palanker, D. Implantation of Modular Photovoltaic Subretinal Prosthesis. Ophthalmic Surg. Lasers Imaging Retin. 2016, 47, 171–174. [Google Scholar] [CrossRef]
- Hayes, M.J.; Burgoyne, T.; Wavre-Shapton, S.T.; Tolmachova, T.; Seabra, M.C.; Futter, C.E. Remodeling of the Basal Labyrinth of Retinal Pigment Epithelial Cells With Osmotic Challenge, Age, and Disease. Investig. Ophthalmol. Vis. Sci. 2019, 60, 2515–2524. [Google Scholar] [CrossRef]
- Del Cerro, M.; Humayun, M.S.; Sadda, S.R.; Cao, J.; Hayashi, N.; Green, W.R.; Del Cerro, C.; De Juan, E. Histologic correlation of human neural retinal transplantation. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3142–3148. [Google Scholar]
- Liu, Z.; Yu, N.; Holz, F.G.; Yang, F.; Stanzel, B.V. Enhancement of retinal pigment epithelial culture characteristics and subretinal space tolerance of scaffolds with 200 nm fiber topography. Biomaterials 2014, 35, 2837–2850. [Google Scholar] [CrossRef]
- Johnson, L.V.; Forest, D.L.; Banna, C.D.; Radeke, C.M.; Maloney, M.A.; Hu, J.; Spencer, C.N.; Walker, A.M.; Tsie, M.S.; Bok, D.; et al. Cell culture model that mimics drusen formation and triggers complement activation associated with age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2011, 108, 18277–18282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.C.; Wyss, U.P.; Pichora, D.; Goosen, M.F.A. An Investigation of Poly(Lactic Acid) Degradation. J. Bioact. Compat. Polym. 1994, 9, 80–100. [Google Scholar] [CrossRef]
- Landes, C.A.; Ballon, A.; Roth, C. Maxillary and mandibular osteosyntheses with PLGA and P(L/DL)LA implants: A 5-year inpatient biocompatibility and degradation experience. Plast. Reconstr. Surg. 2006, 117, 2347–2360. [Google Scholar] [CrossRef] [PubMed]
- Lehtonen, T.J.; Tuominen, J.U.; Hiekkanen, E. Resorbable composites with bioresorbable glass fibers for load-bearing applications. In vitro degradation and degradation mechanism. Acta Biomater. 2013, 9, 4868–4877. [Google Scholar] [CrossRef]
- Weir, N.A.; Buchanan, F.J.; Orr, J.F.; Dickson, G.R. Degradation of poly-L-lactide. Part 1: In vitro and in vivo physiological temperature degradation. Proc. Inst. Mech. Eng. H 2004, 218, 307–319. [Google Scholar] [CrossRef]
- Stanzel, B.V.; Liu, Z.; Somboonthanakij, S.; Wongsawad, W.; Brinken, R.; Eter, N.; Corneo, B.; Holz, F.G.; Temple, S.; Stern, J.H.; et al. Human RPE stem cells grown into polarized RPE monolayers on a polyester matrix are maintained after grafting into rabbit subretinal space. Stem Cell Rep. 2014, 2, 64–77. [Google Scholar] [CrossRef] [Green Version]
- Fronk, A.H.; Vargis, E. Methods for culturing retinal pigment epithelial cells: A review of current protocols and future recommendations. J. Tissue Eng. 2016, 7, 2041731416650838. [Google Scholar] [CrossRef] [Green Version]
- Rizzolo, L.J. Barrier properties of cultured retinal pigment epithelium. Exp. Eye Res. 2014, 126, 16–26. [Google Scholar] [CrossRef]
- Chao, J.R.; Lamba, D.A.; Klesert, T.R.; La Torre, A.; Hoshino, A.; Taylor, R.J.; Jayabalu, A.; Engel, A.L.; Khuu, T.; Wang, R.; et al. Transplantation of Human Embryonic Stem Cell-Derived Retinal Cells into the Subretinal Space of a Non-Human Primate. Transl. Vis. Sci. Technol. 2017, 6, 4. [Google Scholar] [CrossRef]
- Limnios, I.J.; Chau, Y.Q.; Skabo, S.J.; Surrao, D.C.; O’Neill, H.C. Efficient differentiation of human embryonic stem cells to retinal pigment epithelium under defined conditions. Stem Cell Res. Ther. 2021, 12, 248. [Google Scholar] [CrossRef]
- Plaza Reyes, A.; Petrus-Reurer, S.; Padrell Sánchez, S.; Kumar, P.; Douagi, I.; Bartuma, H.; Aronsson, M.; Westman, S.; Lardner, E.; André, H.; et al. Identification of cell surface markers and establishment of monolayer differentiation to retinal pigment epithelial cells. Nat. Commun. 2020, 11, 1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, G.; Seiler, M.J.; Thomas, B.B.; Wu, K.; Radosevich, M.; Sadda, S.R. Revisiting nestin expression in retinal progenitor cells in vitro and after transplantation in vivo. Exp. Eye Res. 2007, 84, 1047–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Li, Y.; Cui, Y.; Roberts, C.; Lu, M.; Wilhelmsson, U.; Pekny, M.; Chopp, M. Beneficial effects of gfap/vimentin reactive astrocytes for axonal remodeling and motor behavioral recovery in mice after stroke. Glia 2014, 62, 2022–2033. [Google Scholar] [CrossRef] [PubMed]
- Qu, L.; Gao, L.; Xu, H.; Duan, P.; Zeng, Y.; Liu, Y.; Yin, Z.Q. Combined transplantation of human mesenchymal stem cells and human retinal progenitor cells into the subretinal space of RCS rats. Sci. Rep. 2017, 7, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Nawaiseh, S.; Thieltges, F.; Liu, Z.; Strack, C.; Brinken, R.; Braun, N.; Wolschendorf, M.; Maminishkis, A.; Eter, N.; Stanzel, B.V. A Step by Step Protocol for Subretinal Surgery in Rabbits. J. Vis. Exp. JoVE 2016, 115, e53927. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, J.K.; Mano, F.; Iezzi, R.; LoBue, S.A., Jr.; Holman, B.H.; Fautsch, M.P.; Olsen, T.W.; Pulido, J.S.; Marmorstein, A.D. Fibrin hydrogels are safe, degradable scaffolds for sub-retinal implantation. PLoS ONE 2020, 15, e0227641. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, J.K.; Manzar, Z.; Bachman, L.A.; Andrews-Pfannkoch, C.; Knudsen, T.; Hill, M.; Schmidt, H.; Iezzi, R.; Pulido, J.S.; Marmorstein, A.D. Fibrin hydrogels as a xenofree and rapidly degradable support for transplantation of retinal pigment epithelium monolayers. Acta Biomater. 2018, 67, 134–146. [Google Scholar] [CrossRef]
- Liu, Z.; Parikh, B.H.; Tan, Q.S.W.; Wong, D.S.L.; Ong, K.H.; Yu, W.; Seah, I.; Holder, G.E.; Hunziker, W.; Tan, G.S.; et al. Surgical Transplantation of Human RPE Stem Cell-Derived RPE Monolayers into Non-Human Primates with Immunosuppression. Stem Cell Rep. 2021, 16, 237–251. [Google Scholar] [CrossRef]
- Fernandes, R.A.B.; Stefanini, F.R.; Falabella, P.; Koss, M.J.; Wells, T.; Diniz, B.; Ribeiro, R.; Schor, P.; Maia, M.; Penha, F.M.; et al. Development of a new tissue injector for subretinal transplantation of human embryonic stem cell derived retinal pigmented epithelium. Int. J. Retin. Vitr. 2017, 3, 41. [Google Scholar] [CrossRef] [Green Version]
- Rauer, O.; Ghosh, F. Survival of full-thickness retinal xenotransplants without immunosuppression. Graefes Arch. Clin. Exp. Ophthalmol. 2001, 239, 145–151. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pig Number | Time of Euthanasia (Weeks) | Right Eye | Left Eye | Time of OCT Scans and Fundus Photography (Weeks) |
|---|---|---|---|---|
| 4 (T149) | 1 | Treated eye | Control eye | 1 |
| 1 (T141) | 2 | Treated eye * | Treated eye | 1, 2 |
| 3 (T146) | 6 | Treated eye | Control eye | 1, 2, 6 |
| 6 (T192) | 6 | Treated eye | Control eye | 1, 2, 6 |
| 5 (T145A) | 8 | Treated eye | Control eye | 1, 2, 6, 8 |
| Protein | Source | Manufacturer | Working Dilution |
|---|---|---|---|
| HNAA | mAb mouse | Novus Biologicals, UK, Abingdon, (235-1) NBP2-34342-0.1 mg | 1:300 |
| STEM121 | mAb mouse | Takara Bio Inc., Kusatsu, Japan, cat. No. Y40410 | 1:100 |
| Bestrophin | mAb mouse | Santa Cruz Inc., Germany, Heidelberg, cat. No. sc-32792 | 1:50 |
| CRALBP | mAb mouse | Novus Biologicals UK, Abingdon, (B2) cat. No. NB100-74392 | 1:100 |
| Vimentin | mAb mouse | Cell Signaling, (D21H3), USA, cat. No. 5741 | 1:100 |
| GFAP | pAb rabbit | Merck Millipore, Germany, Darmstadt, rabbit polyclonal antibody, cat. No. AB5804, lot No. 2464502 | 1:1000 |
| IbaI, Microglial Marker | mAb mouse | Abcam, Cambridge, UK, mouse monoclonal antibody, cat. No. ab15690, clone 1022-5 | 1:250 |
| PKC alpha | pAb rabbit | Sigma-Aldrich, Germany, Taufkirchen, rabbit polyclonal, cat. No. P4334 | 1:10,000 |
| Lectin PNA Conjugate Alexa Fluor 488 | Molecular probes, cat. No. L-21409 | 1:300 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lytvynchuk, L.; Ebbert, A.; Studenovska, H.; Nagymihály, R.; Josifovska, N.; Rais, D.; Popelka, Š.; Tichotová, L.; Nemesh, Y.; Čížková, J.; et al. Subretinal Implantation of Human Primary RPE Cells Cultured on Nanofibrous Membranes in Minipigs. Biomedicines 2022, 10, 669. https://doi.org/10.3390/biomedicines10030669
Lytvynchuk L, Ebbert A, Studenovska H, Nagymihály R, Josifovska N, Rais D, Popelka Š, Tichotová L, Nemesh Y, Čížková J, et al. Subretinal Implantation of Human Primary RPE Cells Cultured on Nanofibrous Membranes in Minipigs. Biomedicines. 2022; 10(3):669. https://doi.org/10.3390/biomedicines10030669
Chicago/Turabian StyleLytvynchuk, Lyubomyr, Annabelle Ebbert, Hana Studenovska, Richárd Nagymihály, Natasha Josifovska, David Rais, Štěpán Popelka, Lucie Tichotová, Yaroslav Nemesh, Jana Čížková, and et al. 2022. "Subretinal Implantation of Human Primary RPE Cells Cultured on Nanofibrous Membranes in Minipigs" Biomedicines 10, no. 3: 669. https://doi.org/10.3390/biomedicines10030669