
Microwaves as Diagnostic Tool for Pituitary Tumors: Preliminary Investigations

 ,
,  ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Physiopathology and Problem Description
3. Methods
3.1. Forward Problem
3.2. Inverse Problem
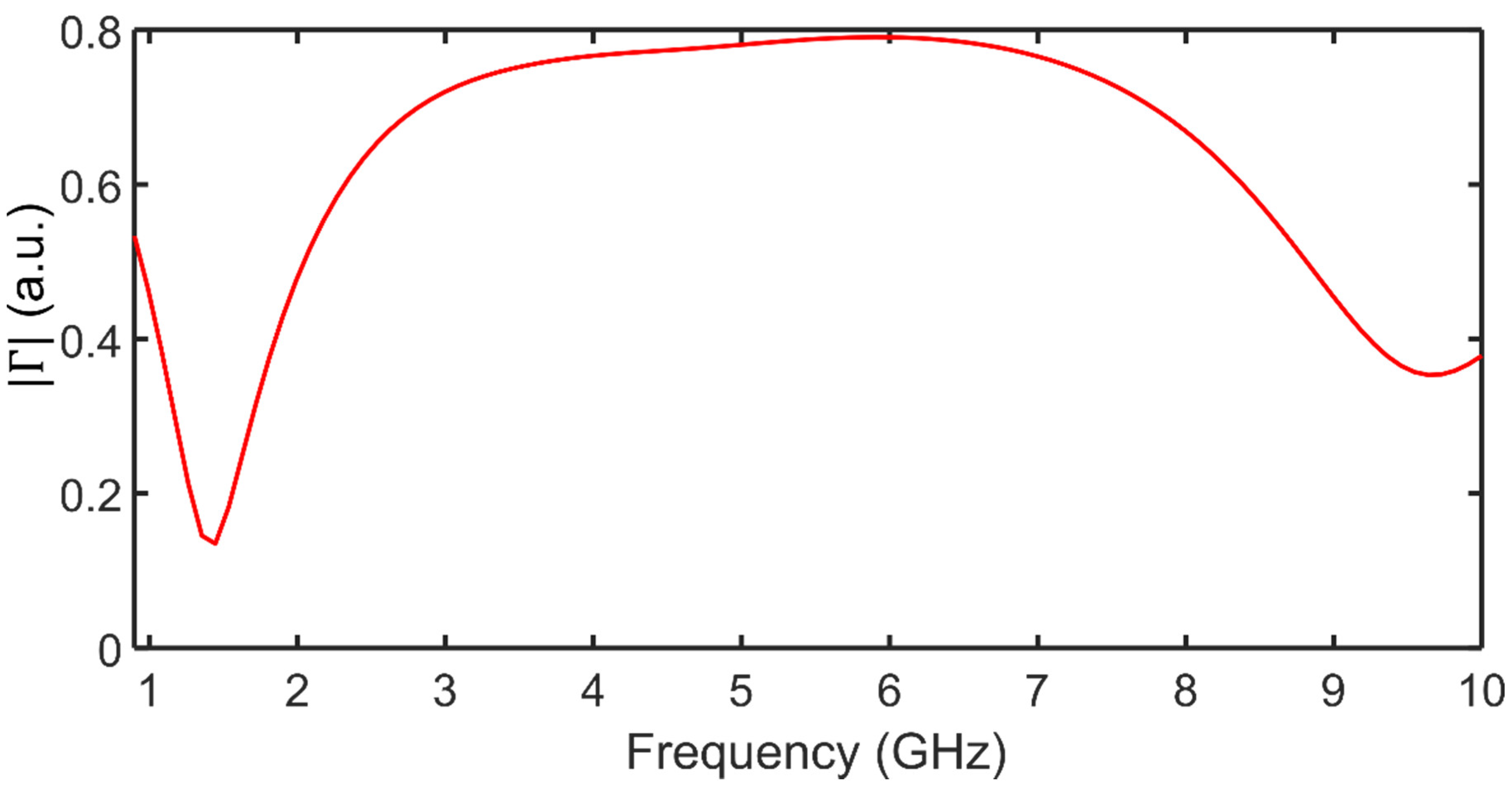
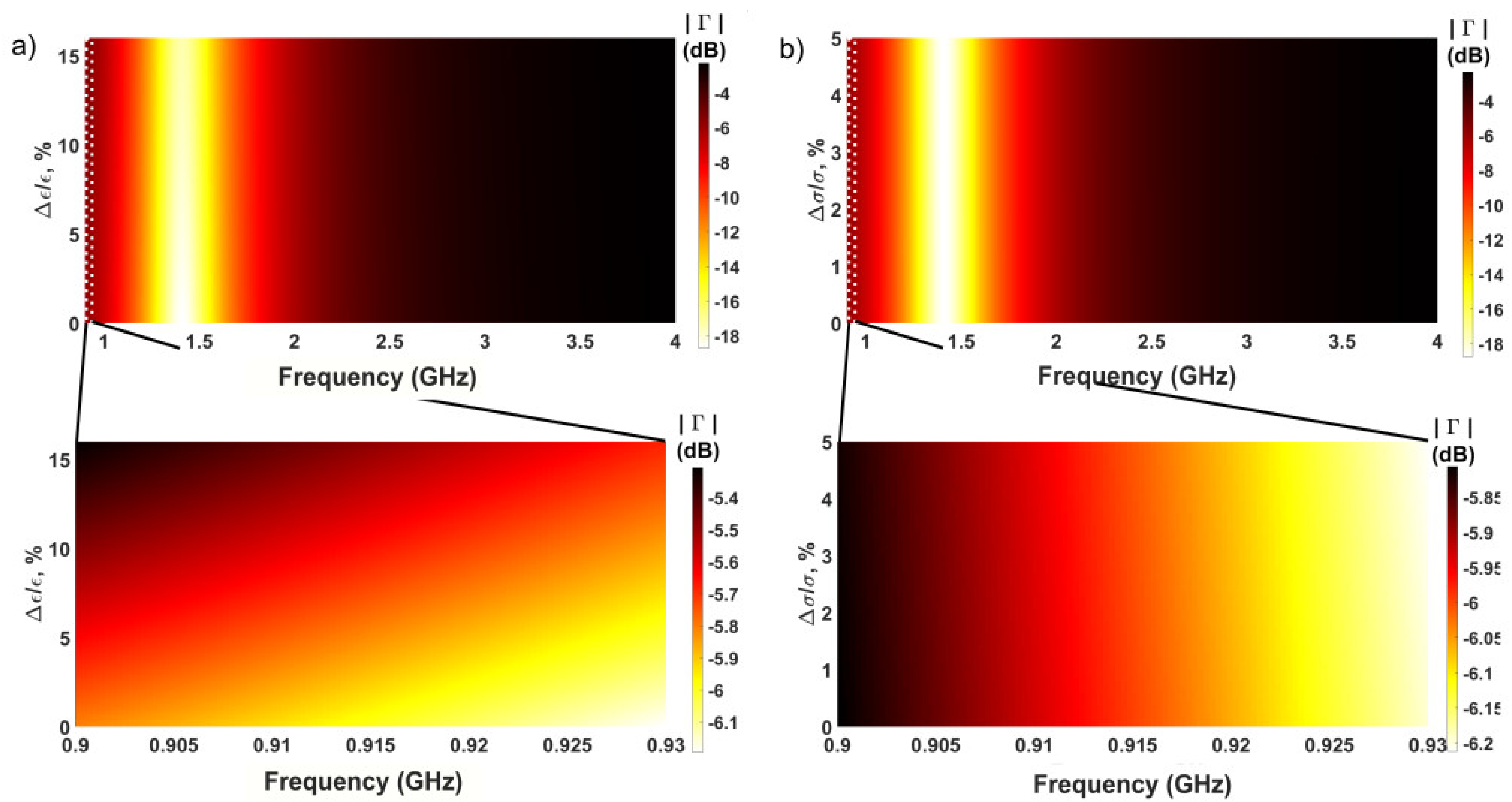
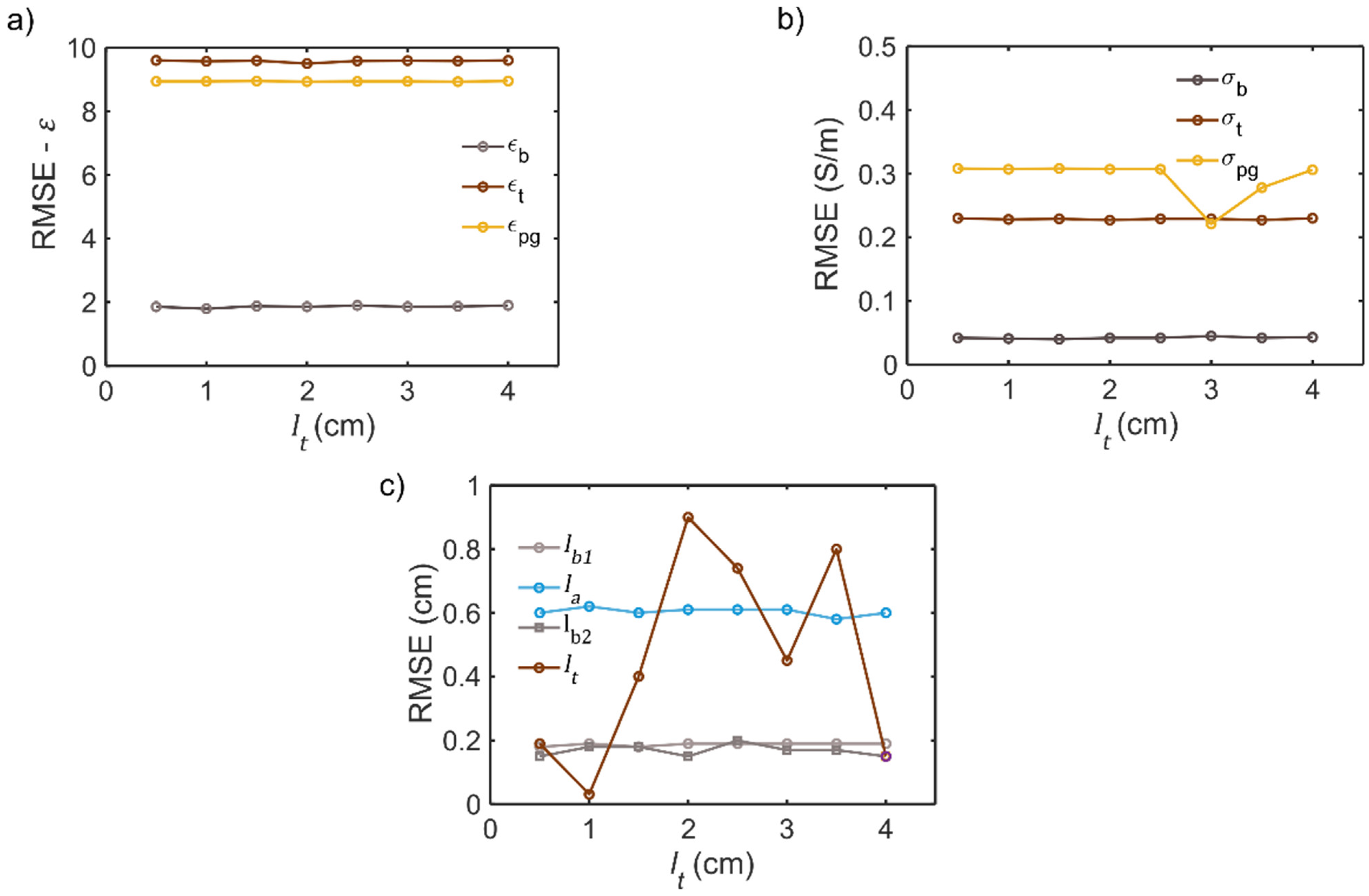
4. Results
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations and Acronyms
| Computerized Tomography | CT |
| Electromagnetic Fields | EMF |
| Finite Difference Time Domain | FDTD |
| Genetic Algorithm | GA |
| Industrial, Scientific and Medical | ISM |
| Magnetic Resonance Imaging | MRI |
| Microwaves | MW |
| Nuclear Magnetic Resonance | NMR |
| Root Mean Square Error | RMSE |
| Trans-Sphenoidal Approach | TSSPA |
List of Symbols and Variables
| Variable/Symbol | Description | Unit |
| Broadening parameter | - | |
| Speed of light | m/s | |
| Penetration depth | m | |
| Relative dielectric permittivity | - | |
| Air dielectric permittivity | - | |
| Vacuum permittivity | F/m | |
| Bone dielectric permittivity | - | |
| Pituitary tumor dielectric permittivity | - | |
| Pituitary gland dielectric permittivity | - | |
| Real part of the complex permittivity | - | |
| Imaginary part of the complex permittivity | - | |
| Permittivity at optical frequency | - | |
| Dielectric strength | - | |
| Static dielectric permittivity | - | |
| Working frequency | GHz | |
| Reflection coefficient | - | |
| Complex propagation constant | 1/m | |
| Length of the anterior sphenoidal sinus | mm | |
| Size of the air gap | mm | |
| Length of the posterior sinus | mm | |
| Size of the pituitary tumor | mm | |
| Number of layers | - | |
| Number of frequencies | - | |
| Number of unknowns | - | |
| Electrical conductivity of air | S/m | |
| Electrical conductivity of bone tissue | S/m | |
| Electrical conductivity of pituitary tumor | S/m | |
| Electrical conductivity of pituitary gland | S/m | |
| Relaxation time | ps | |
| Angular frequency | rad/s | |
| Characteristic impedance of the q-th medium | Ω | |
| Input impedance of the q-th medium | Ω | |
| Vacuum characteristic impedance | Ω |
References
- Gasperi, M.; The Acromegaly Study Group of the Italian Society of Endocrinology; Martino, E.; Manetti, L.; Arosio, M.; Porretti, S.; Faglia, G.; Mariotti, S.; Colao, A.M.; Lombardi, G.; et al. Prevalence of thyroid diseases in patients with acromegaly: Results of an Italian multi-center study. J. Endocrinol. Investig. 2002, 25, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Filopanti, M.; Barbieri, A.M.; Angioni, A.R.; Colao, A.; Gasco, V.; Grottoli, S.; Peri, A.; Baglioni, S.; Fustini, M.F.; Pigliaru, F.; et al. Dopamine D 2 Receptor gene polymorphisms and response to cabergoline therapy in patients with prolactin-secreting pituitary adenomas. Pharm. J. 2008, 8, 357–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campero, A.; Martins, C.; Yasuda, A.; Rhoton, A.L., Jr. Microsurgical anatomy of the diaphragma sellae and its role in directing the pattern of growth of pituitary adenomas. Neurosurgery 2008, 62, 717–723. [Google Scholar] [PubMed]
- Serioli, S.; Doglietto, F.; Fiorindi, A.; Biroli, A.; Mattavelli, D.; Buffoli, B.; Ferrari, M.; Cornali, C.; Rodella, L.; Maroldi, R.; et al. Pituitary adenomas and invasiveness from anatomo-surgical, radiological, and histological perspectives: A systematic literature review. Cancers 2019, 11, 1936. [Google Scholar]
- Tortora, F.; Negro, A.; Grasso, L.F.; Colao, A.; Pivonello, R.; Splendiani, A.; Brunese, L.; Caranci, F. Pituitary magnetic resonance imaging predictive role in the therapeutic response of growth hormone-secreting pituitary adenomas. Gland. Surg. 2019, 8, S150–S158. [Google Scholar] [CrossRef]
- Casanueva, F.F.; Barkan, A.L.; Buchfelder, M.; Klibanski, A.; Laws, E.R.; Loeffler, J.S.; Melmed, S.; Mortini, P.; Wass, J.; Giustina, A. Criteria for the definition of Pituitary Tumor Centers of Excellence (PTCOE): A Pituitary Society statement. Pituitary 2017, 20, 489–498. [Google Scholar] [CrossRef]
- Daly, A.F.; Beckers, A. The epidemiology of pituitary adenomas. Endocrinol Metab Clin. N. Am. 2020, 49, 347–355. [Google Scholar]
- Bell, R.A. Economics of MRI technology. J. Magn. Reson. Imaging 1996, 6, 10–25. [Google Scholar]
- Robinson, J.C.; Whaley, C.; Brown, T.T. Reference pricing, consumer cost-sharing, and insurer spending for advanced imaging tests. Med. Care 2016, 54, 1050–1055. [Google Scholar] [CrossRef]
- Callahan, M.J.; MacDougall, R.D.; Bixby, S.D.; Voss, S.D.; Robertson, R.L.; Cravero, J.P. Ionizing radiation from computed tomography versus anesthesia for magnetic resonance imaging in infants and children: Patient safety considerations. Pediatr. Radiol. 2018, 48, 21–30. [Google Scholar]
- Chandra, R.; Zhou, H.; Balasingham, I.; Narayanan, R.M. On the opportunities and challenges in microwave medical sensing and imaging. IEEE Trans. Biomed. Eng. 2015, 62, 1667–1682. [Google Scholar] [CrossRef]
- Shao, W.; McCollough, T. Advances in microwave near-field imaging: Prototypes, systems, and applications. IEEE Microw. Mag. 2020, 21, 94–119. [Google Scholar] [CrossRef]
- Larsen, L.E.; Jacobi, J.H. Medical Applications of Microwave Imaging; IEEE Press: New York, NY, USA, 1985. [Google Scholar]
- Pastorino, M.; Randazzo, A. Microwave Imaging Methods and Applications, 1st ed.; Artech House: Boston, MA, USA, 2018. [Google Scholar]
- Nikolova, N.K. Microwave imaging for breast cancer. IEEE Microw. Mag. 2011, 12, 78–94. [Google Scholar] [CrossRef]
- Di Meo, S.; Espin-Lopez, P.F.; Martellosio, A.; Pasian, M.; Matrone, G.; Bozzi, M.; Magenes, G.; Mazzanti, A.; Perregrini, L.; Svelto, F.; et al. On the feasibility of breast cancer imaging systems at millimeter-waves frequencies. IEEE Trans. Microw. Theory Technol. 2017, 65, 1795–1806. [Google Scholar] [CrossRef]
- Islam, M.; Mahmud, M.; Islam, M.T.; Kibria, S.; Samsuzzaman, M. A low cost and portable microwave imaging system for breast tumor detection using UWB directional antenna array. Sci. Rep. 2019, 9, 15491. [Google Scholar]
- Aldhaeebi, M.A.; Alzoubi, K.; Almoneef, T.S.; Bamatraf, S.M.; Attia, H.; Ramahi, O.M. Review of microwaves techniques for breast cancer detection. Sensors 2020, 20, 2390. [Google Scholar] [CrossRef] [Green Version]
- Hosseinzadegan, S.; Fhager, A.; Persson, M.; Geimer, S.D.; Meaney, P.M. Discrete dipole approximation-based microwave tomography for fast breast cancer imaging. IEEE Trans. Microw. Theory Tech. 2021, 69, 2741–2752. [Google Scholar] [CrossRef]
- Scapaticci, R.; Di Donato, L.; Catapano, I.; Crocco, L. A feasibility study on microwave imaging for brain stroke monitoring. Prog. Electromagn. Res. B 2012, 40, 305–324. [Google Scholar] [CrossRef] [Green Version]
- Tournier, P.H.; Bonazzoli, M.; Dolean, V.; Rapetti, F.; Hecht, F.; Nataf, F.; Aliferis, I.; El Kanfoud, I.; Migliaccio, C.; De Buhan, M.; et al. Numerical modeling and high-speed par- allel computing: New perspectives on tomographic microwave imaging for brain stroke detection and monitoring. IEEE Antennas Propag. Mag. 2017, 59, 98–110. [Google Scholar] [CrossRef] [Green Version]
- Scapaticci, R.; Bjelogrlic, M.; Tobon-Vasquez, J.; Vipiana, F.; Mattes, M.; Crocco, L. Microwave technology for brain imaging and monitoring: Physical foundations, potential and limitations. In Emerging Electromagnetic Technologies for Brain Diseases Diagnostics, Monitoring and Therapy, 1st ed.; Crocco, L., Karanasiou, I., James, M.L., Conceição, R.C., Eds.; Springer International Publishing AG: Berlin, Germany, 2018; pp. 7–35. [Google Scholar]
- Bisio, I.; Estatico, C.; Fedeli, A.; Lavagetto, F.; Pastorino, M.; Randazzo, A.; Sciarrone, A. Variable-exponent Lebesgue-space inversion for brain stroke microwave imaging. IEEE Trans. Microw. Theory Tech. 2020, 68, 1882–1895. [Google Scholar] [CrossRef]
- Al-Saffar, A.; Bialkowski, A.; Baktashmotlagh, M.; Trakic, A.; Guo, L.; Abbosh, A. Closing the gap of simulation to reality in electromagnetic imaging of brain strokes via deep neural networks. IEEE Trans. Comp. Imaging 2021, 7, 13–21. [Google Scholar] [CrossRef]
- Ruvio, G.; Cuccaro, A.; Solimene, R.; Brancaccio, A.; Basile, B.; Amman, M.J. Microwave bone imaging: A preliminary scanning system for proof-of-concept. Healthc. Technol. Lett. 2016, 3, 218–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahdi Rezaeieh, S.; Zamani, A.; Bialkowski, K.S.; Abbosh, A.M. Novel Microwave Torso Scanner for Thoracic Fluid Accumulation Diagnosis and Monitoring. Sci. Rep. 2017, 7, 304. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.J.; Liu, J.X.; Ye, Q.Y. Research on the detection of the brain tumor with the ultrawide-band microwave signal based on the high- precision symplectic finite-difference time-domain electromagnetic algorithm and beam forming imaging algorithm. Int. J. RF Microw. Comput. Aided Eng. 2020, 30, e22463. [Google Scholar] [CrossRef]
- Dachena, C.; Fedeli, A.; Fanti, A.; Lodi, M.B.; Pastorino, M.; Randazzo, A. Microwave Imaging for the Diagnosis of Cervical Diseases: A Feasibility Analysis. IEEE J. Electromagn. RF Microw. Med. Biol. 2021, 5, 277–285. [Google Scholar] [CrossRef]
- Dachena, C.; Fedeli, A.; Fanti, A.; Lodi, M.B.; Fumera, G.; Randazzo, A.; Pastorino, M. Microwave Imaging of the Neck by Means of Artificial Neural Networks for Tumor Detection. IEEE Open J. Antennas Propag. 2021, 2, 1044–1056. [Google Scholar] [CrossRef]
- Zada, G.; Kelly, D.F.; Cohan, P.; Wang, C.; Swerdloff, R. Endonasal transsphenoidal approach to treat pituitary adenomas and other sellar lesions: An assessment of efficacy, safety, and patient impressions of the surgery. J. Neurosurg. 2003, 98, 350–358. [Google Scholar] [CrossRef]
- Penn, D.L.; Burke, W.T.; Laws, E.R. Management of non-functioning pituitary adenomas: Surgery. Pituitary 2018, 21, 145–153. [Google Scholar]
- Pérez-López, C.; Álvarez-Escolá, C.; Isla Guerrero, A. Therapeutic approach to non-functioning pituitary adenomas. Med. Clínica 2021, 156, 284–289. [Google Scholar]
- Hasgall, P.A.; Neufeld, E.; Gosselin, M.; Klingenbock, A.; Kuster, N. IT’IS Database for Thermal and Electromagnetic Parameters of Biological Tissues. IT’IS Foundation. 2012. Available online: https://itis.swiss/virtual-population/tissue-properties/database (accessed on 4 February 2022).
- Gabriel, S.; Lau, R.; Gabriel, C. The dielectric properties of biological tissues: II. Measurements in the frequency range 10 Hz to 20 GHz. Phys. Med. Biol. 1996, 41, 2251–2269. [Google Scholar] [CrossRef] [Green Version]
- Gavazzi, S.; Limone, P.; De Rosa, G.; Molinari, F.; Vecchi, G. Comparison of microwave dielectric properties of human normal, benign and malignant thyroid tissues obtained from surgeries: A preliminary study. Biomed. Phys. Eng. Express 2018, 4, 47003. [Google Scholar] [CrossRef]
- Orphanidis, S. Electromagnetic Waves and Antennas. 2016, pp. 186–190. Available online: https://www.ece.rutgers.edu/~orfanidi/ewa (accessed on 15 January 2022).
- Massa, R.; Migliore, M.D.; Panariello, G.; Pinchera, D.; Schettino, F.; Caprio, E.; Griffo, R. Wide band permittivity measurements of palm (phoenix canariensis) and rhynchophorus ferrugineus (coleoptera curculionidae) for RF pest control. J. Microw. Power Electromagn. Energy 2014, 48, 158–169. [Google Scholar] [CrossRef]
- Fan, S.; Staebell, K.; Misra, D. Static analysis of an open-ended coaxial line terminated by layered media. IEEE Trans. Instrum. Meas. 1990, 39, 435–437. [Google Scholar] [CrossRef]
- Alanen, E.; Lahtinen, T.; Nuutinen, J. Variational formulation of open-ended coaxial line in contact with layered biological medium. IEEE Trans. Biomed. Eng. 1998, 45, 1241–1248. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]
- Pastorino, M. Stochastic optimization methods applied to microwave imaging: A review. IEEE Trans. Antennas Propag. 2007, 55, 538–548. [Google Scholar] [CrossRef]
- Pastorino, M.; Massa, A.; Caorsi, S. A microwave inverse scattering technique for image reconstruction based on a genetic algorithm. IEEE Trans. Instrum. Meas. 2000, 49, 573–578. [Google Scholar] [CrossRef]
- Guarin, G.; Hofmann, M.; Nehring, J.; Weigel, R.; Fischer, G.; Kissinger, D. Miniature microwave biosensors: Noninvasive applications. IEEE Microw. Mag. 2015, 16, 71–86. [Google Scholar] [CrossRef]
- La Gioia, A.; Santorelli, A.; O’Halloran, M.; Porter, E. Predicting the Sensing Radius of a Coaxial Probe Based on the Probe Dimensions. IEEE Trans. Antennas Propag. 2020, 68, 6704–6716. [Google Scholar] [CrossRef]
- Farshkaran, A.; Porter, E. Improved Sensing Volume Estimates for Coaxial Probes to Measure the Dielectric Properties of Inhomogeneous Tissues. IEEE J. Electromagn. RF Microw. Med. Biol. 2022, Early Access, 1–7. [Google Scholar] [CrossRef]
- Rodriguez-Duarte, D.O.; Vasquez, J.A.T.; Scapaticci, R.; Crocco, L.; Vipiana, F. Assessing a microwave imaging system for brain stroke monitoring via high fidelity numerical modelling. IEEE J. Electromagn. RF Microw. Med. Biol. 2021, 5, 238–245. [Google Scholar] [CrossRef]
- Fedeli, A.; Schenone, V.; Randazzo, A.; Pastorino, M.; Henriksson, T.; Semenov, S. Nonlinear S-Parameters Inversion for Stroke Imaging. IEEE Trans. Microw. Theory Tech. 2020, 69, 1760–1771. [Google Scholar] [CrossRef]
- MiMED. Available online: https://www.cost.eu/actions/TD1301 (accessed on 10 May 2022).
- EMERALD. Available online: https://cordis.europa.eu/project/id/764479 (accessed on 10 May 2022).
- WEBOING. Available online: https://cordis.europa.eu/project/id/793449 (accessed on 10 May 2022).
- MammoWave. Available online: https://cordis.europa.eu/project/id/830265 (accessed on 10 May 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | Unit |
|---|---|---|
| 10.02 | a.u. | |
| 47.24 | a.u. | |
| 11.60 | ps | |
| 0.014 | a.u. | |
| 1.48 | a.u. | |
| 667.57 | ps | |
| 0.95 | a.u. | |
| 0.60 | S/m |
| Parameter | Value (cm) |
|---|---|
| 0.42 | |
| 1.34 | |
| 0.52 | |
| 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casula, F.; Lodi, M.B.; Curreli, N.; Fedeli, A.; Scapaticci, R.; Muntoni, G.; Randazzo, A.; Djuric, N.; Vannucci, L.; Fanti, A. Microwaves as Diagnostic Tool for Pituitary Tumors: Preliminary Investigations. Electronics 2022, 11, 1608. https://doi.org/10.3390/electronics11101608
Casula F, Lodi MB, Curreli N, Fedeli A, Scapaticci R, Muntoni G, Randazzo A, Djuric N, Vannucci L, Fanti A. Microwaves as Diagnostic Tool for Pituitary Tumors: Preliminary Investigations. Electronics. 2022; 11(10):1608. https://doi.org/10.3390/electronics11101608
Chicago/Turabian StyleCasula, Filippo, Matteo Bruno Lodi, Nicola Curreli, Alessandro Fedeli, Rosa Scapaticci, Giacomo Muntoni, Andrea Randazzo, Nikola Djuric, Luca Vannucci, and Alessandro Fanti. 2022. "Microwaves as Diagnostic Tool for Pituitary Tumors: Preliminary Investigations" Electronics 11, no. 10: 1608. https://doi.org/10.3390/electronics11101608