
PHB/CHIT Scaffold as a Promising Biopolymer in the Treatment of Osteochondral Defects—An Experimental Animal Study

 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation and Characterization of Composite Scaffold
2.2. Animals
2.3. Surgical Manipulation with Biopolymer Composites
2.4. Monitoring Phase
2.5. X-ray Examination
2.6. CT Examination
2.7. MRI (Magnetic Resonance Imaging) Examination
2.8. Histology
2.8.1. Hematoxylin-Eosin Staining
2.8.2. Alcian Blue Staining
2.8.3. Safranin-O Staining
2.8.4. Picrosirius Red Staining
2.8.5. Histological Scoring Systems
Pineda Scoring System
O’Driscoll Scoring System
Polarized Microscopy
2.9. Statistical Analyses
3. Results
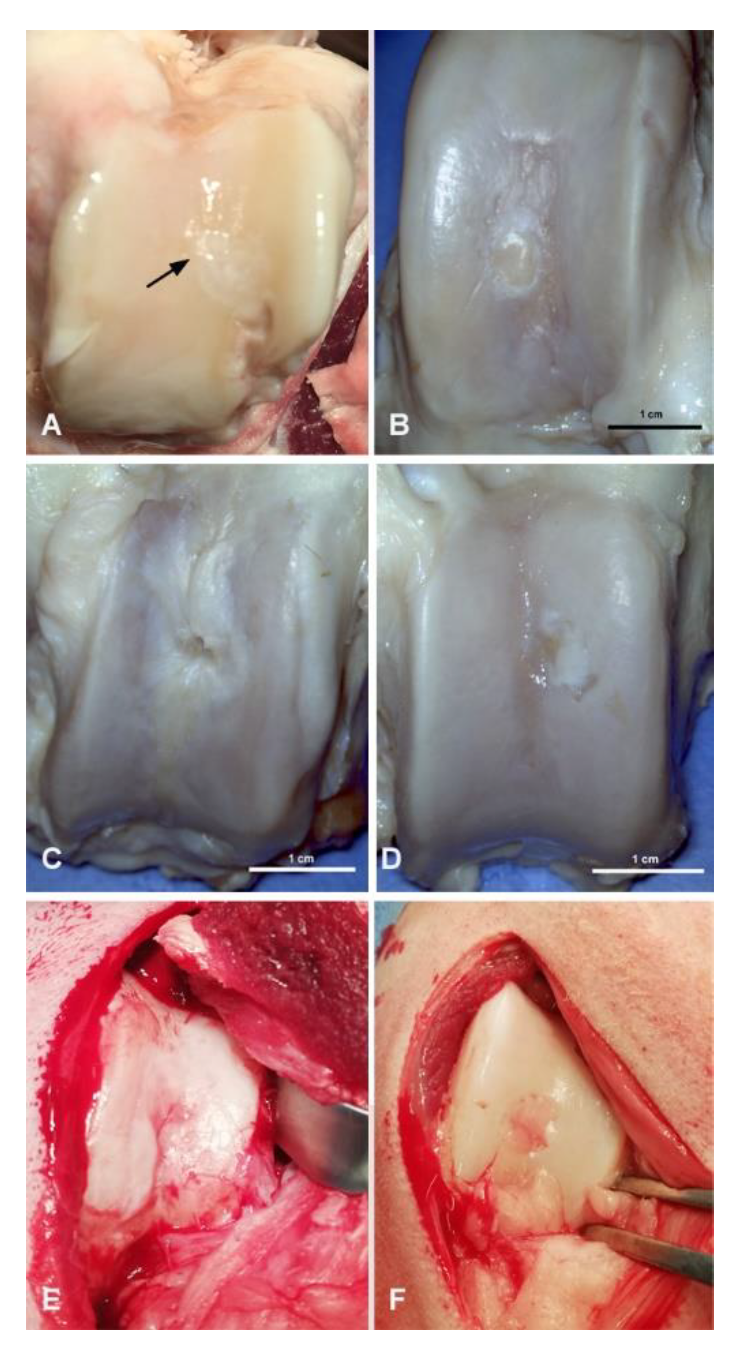
3.1. Macroscopic Evaluation of Repaired Cartilage Defects
3.2. X-ray Evaluation
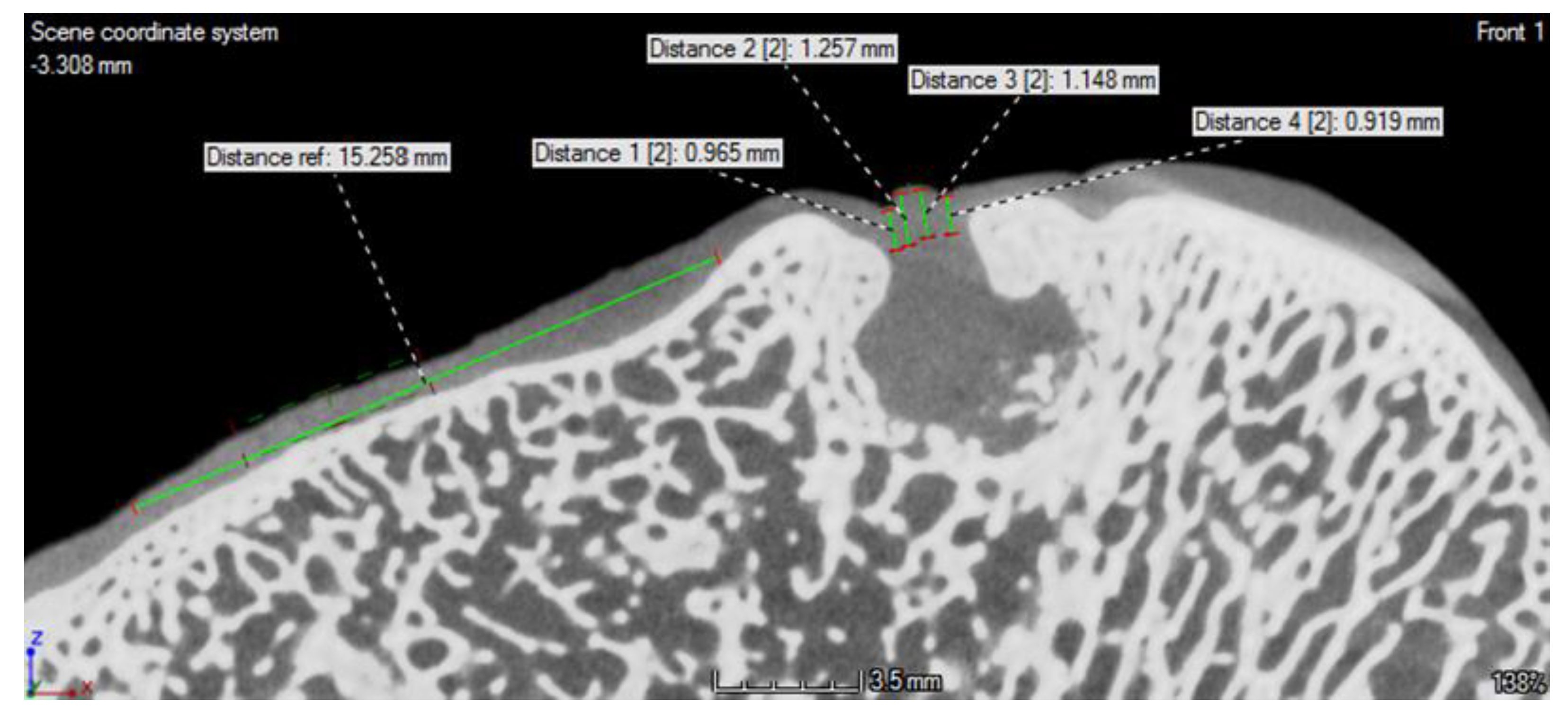
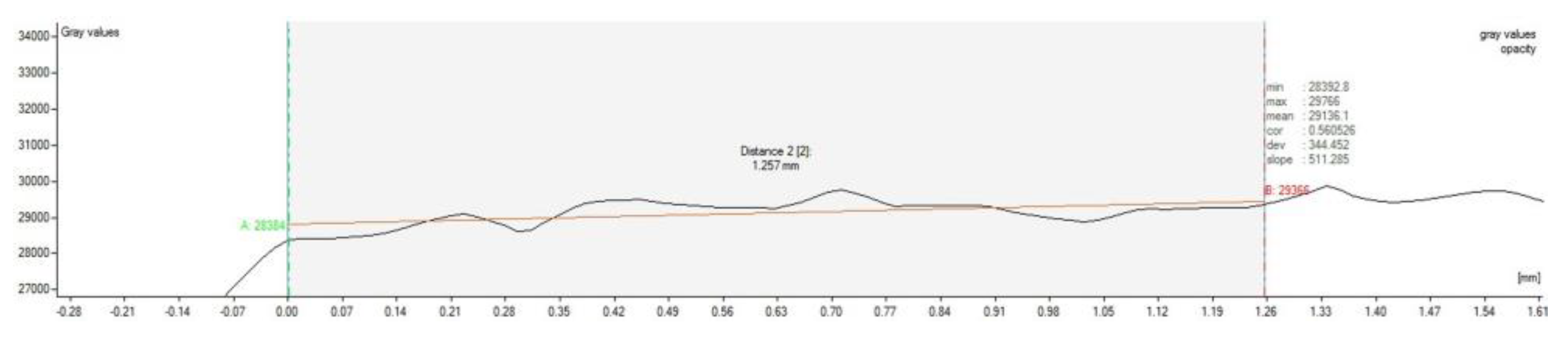
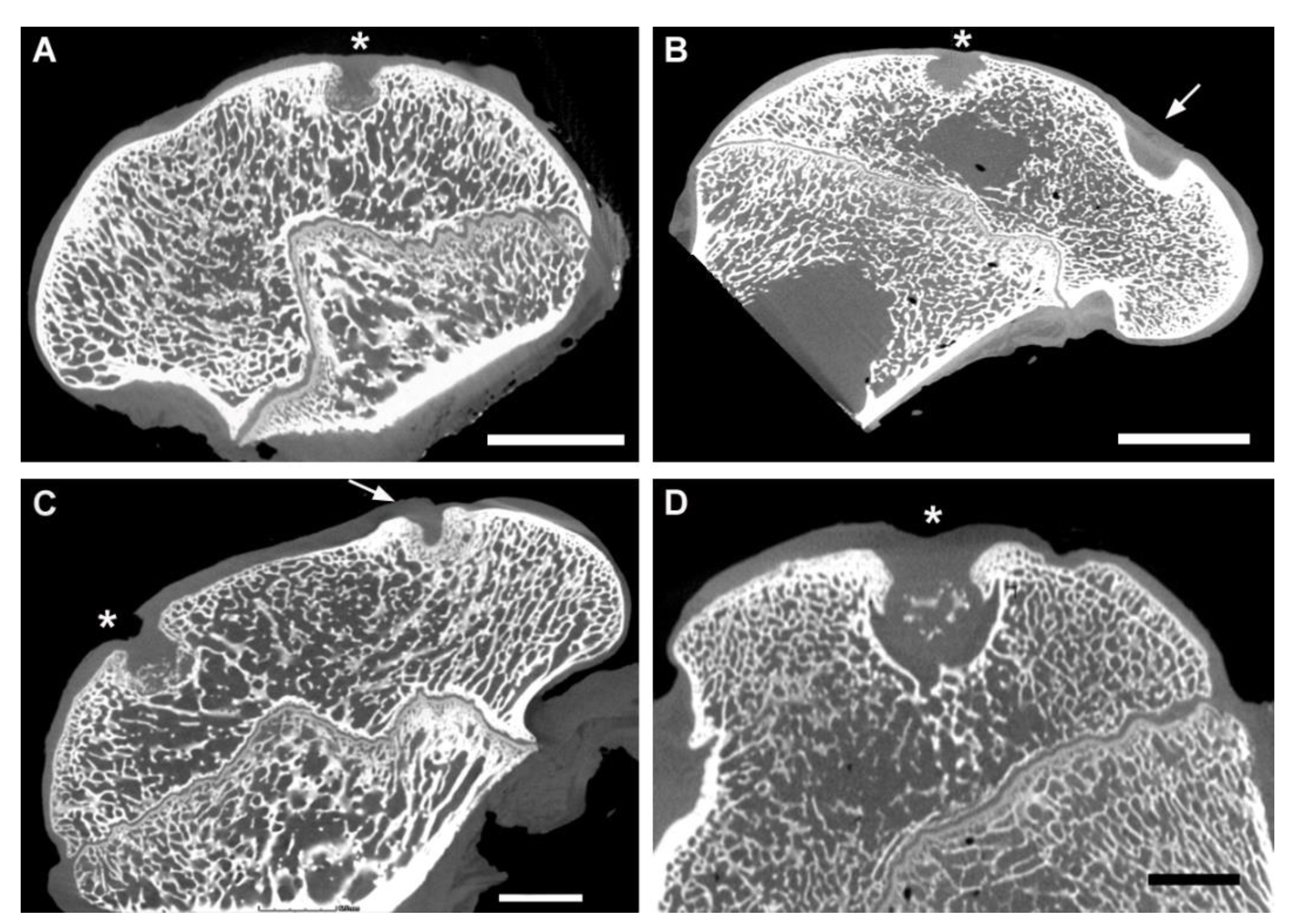
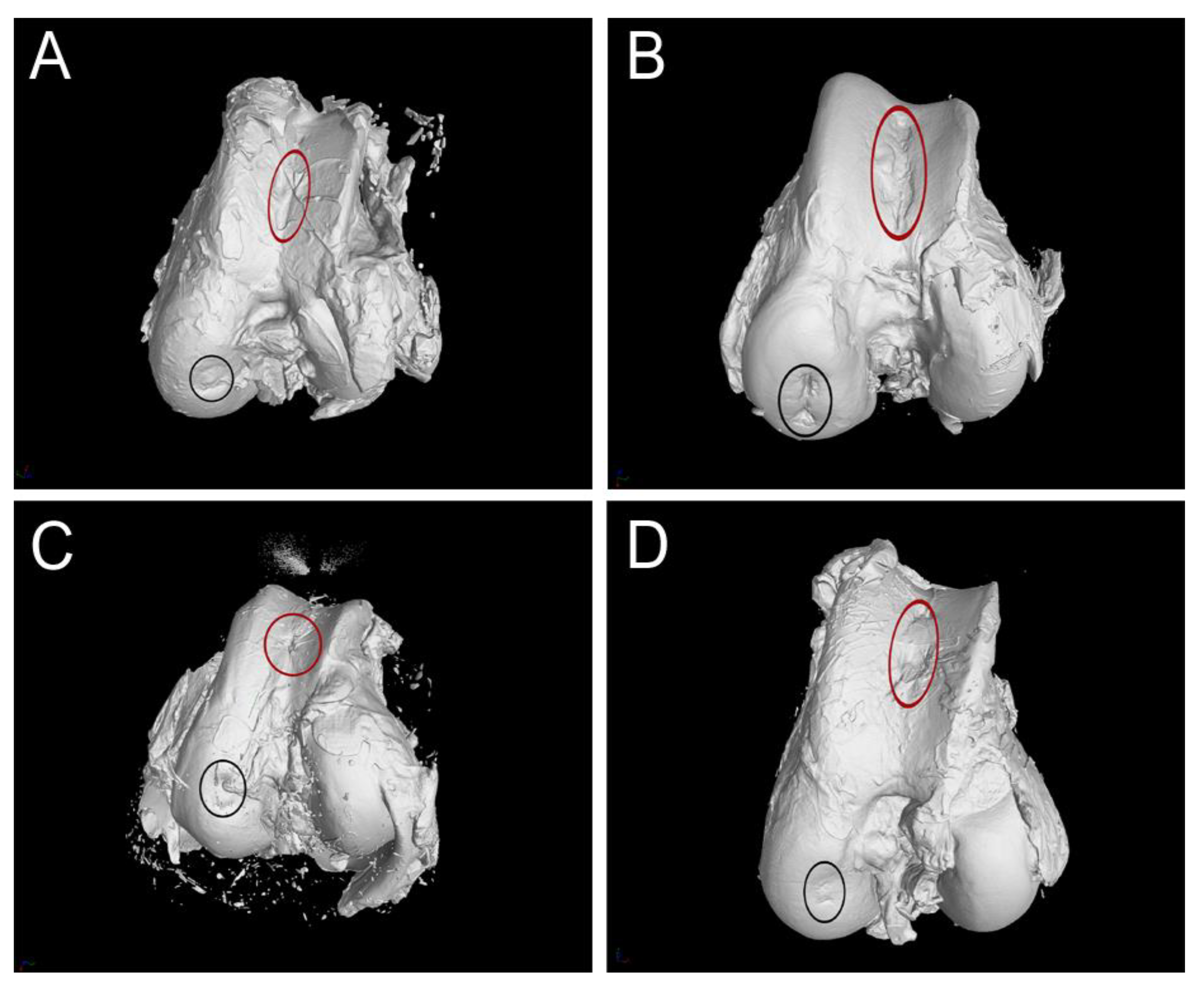
3.3. CT Evaluation
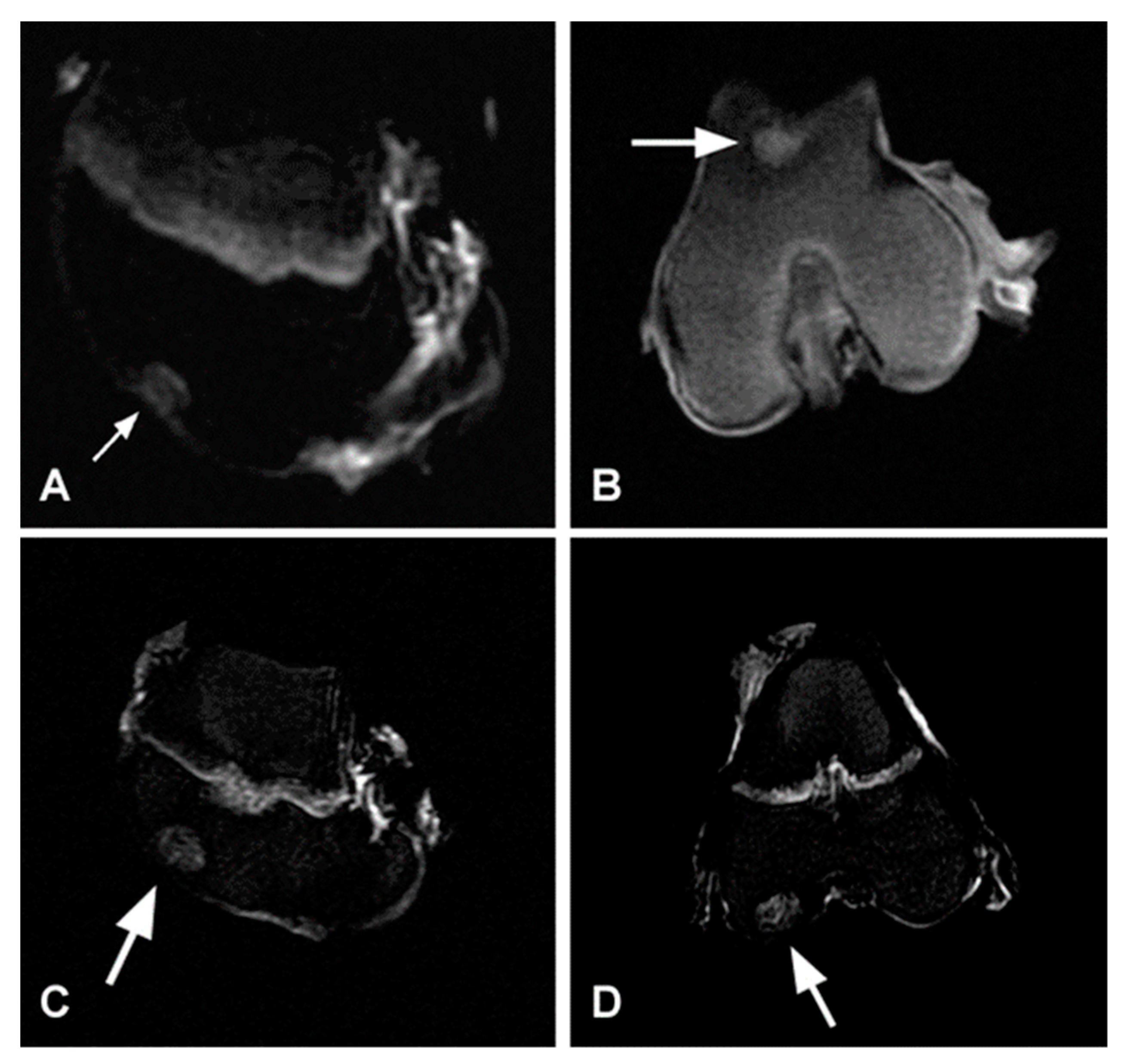
3.4. MRI Evaluation
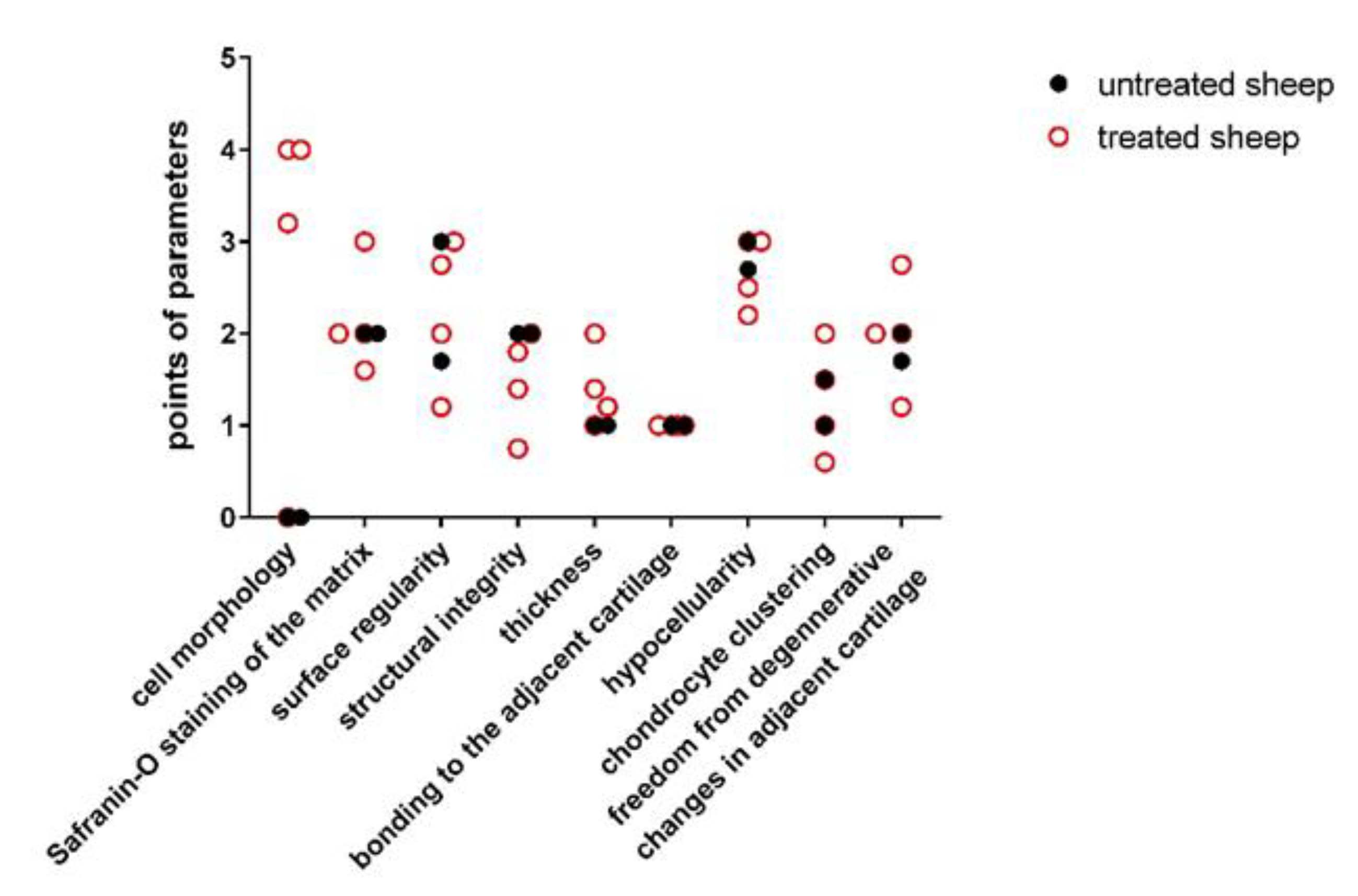
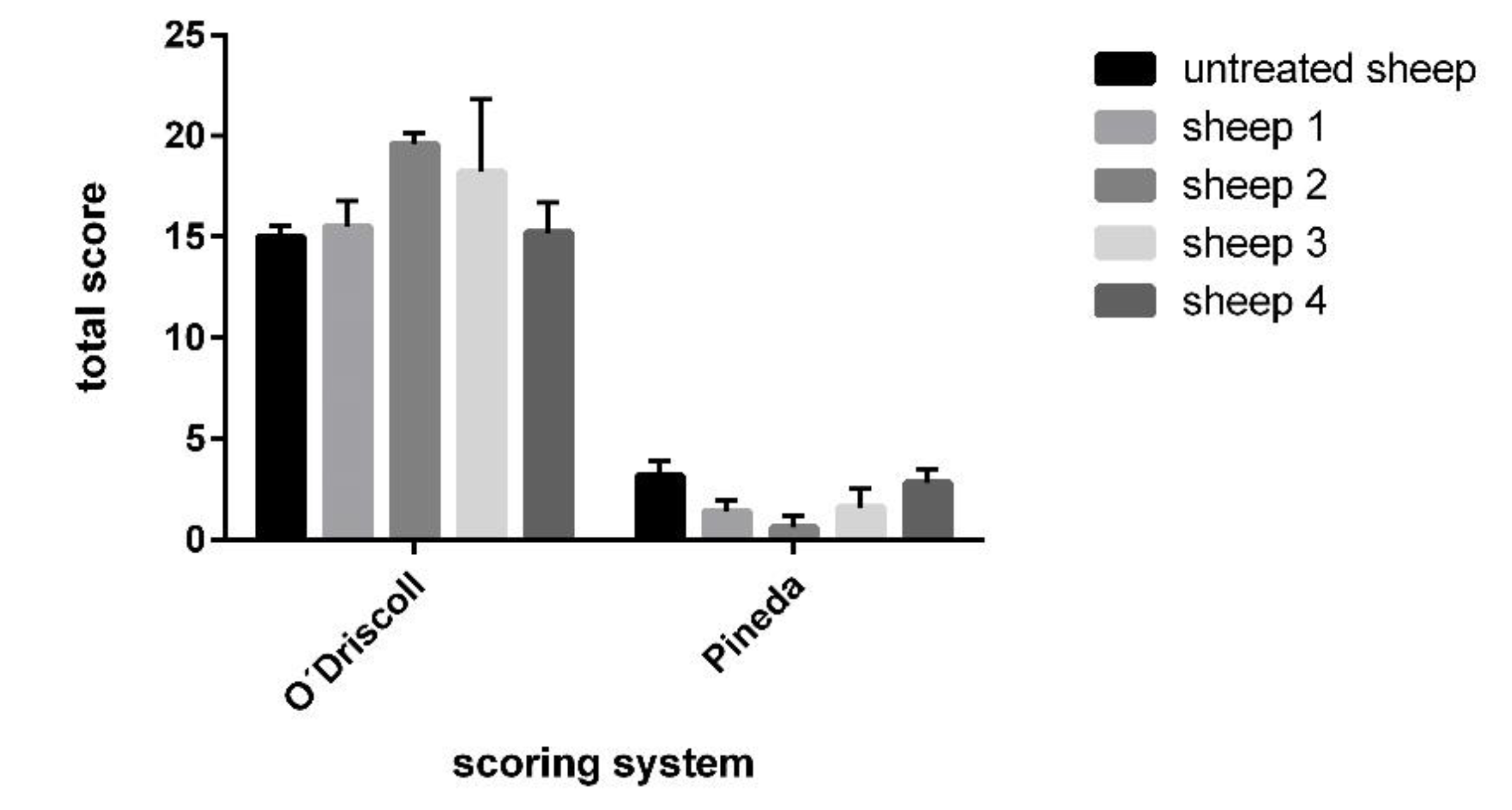
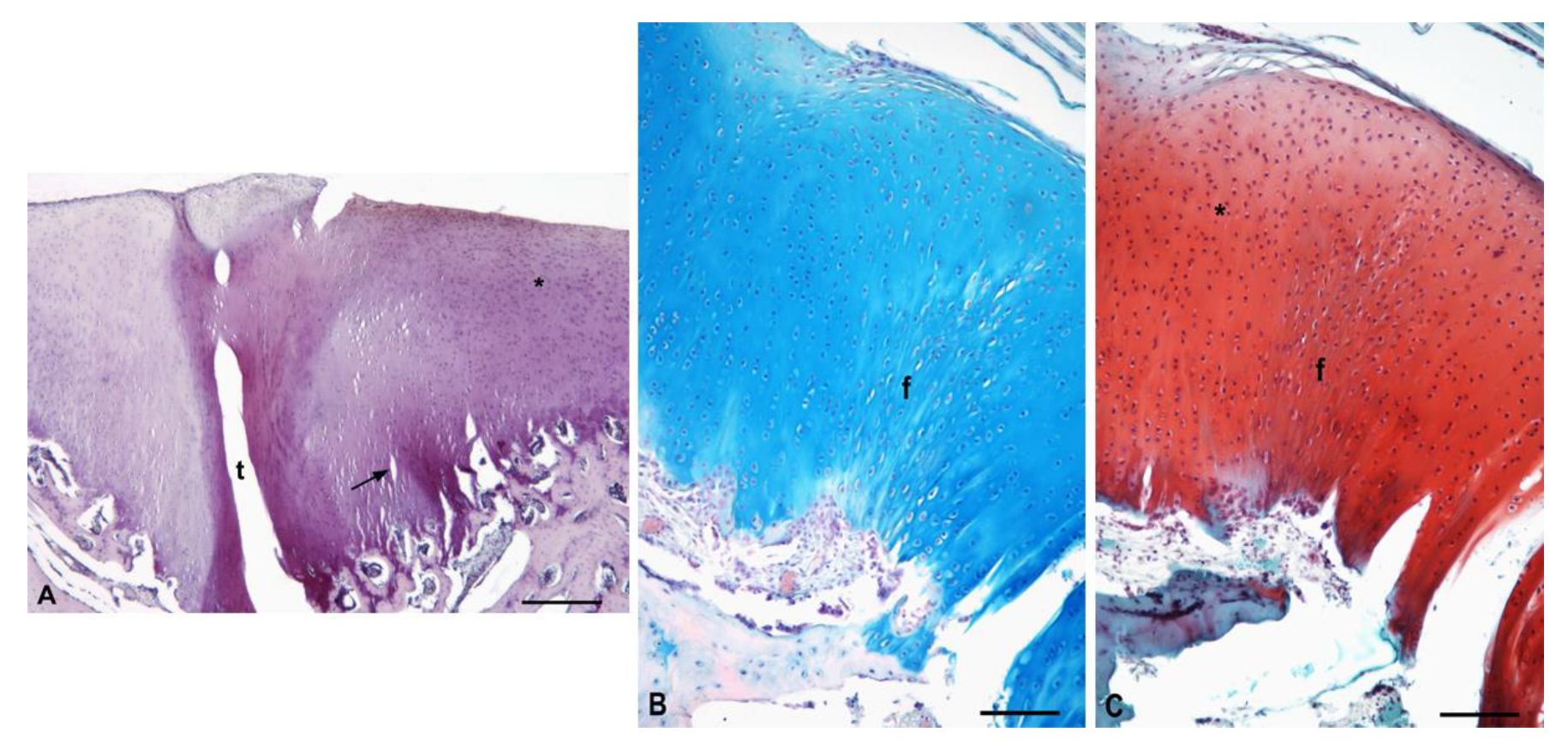
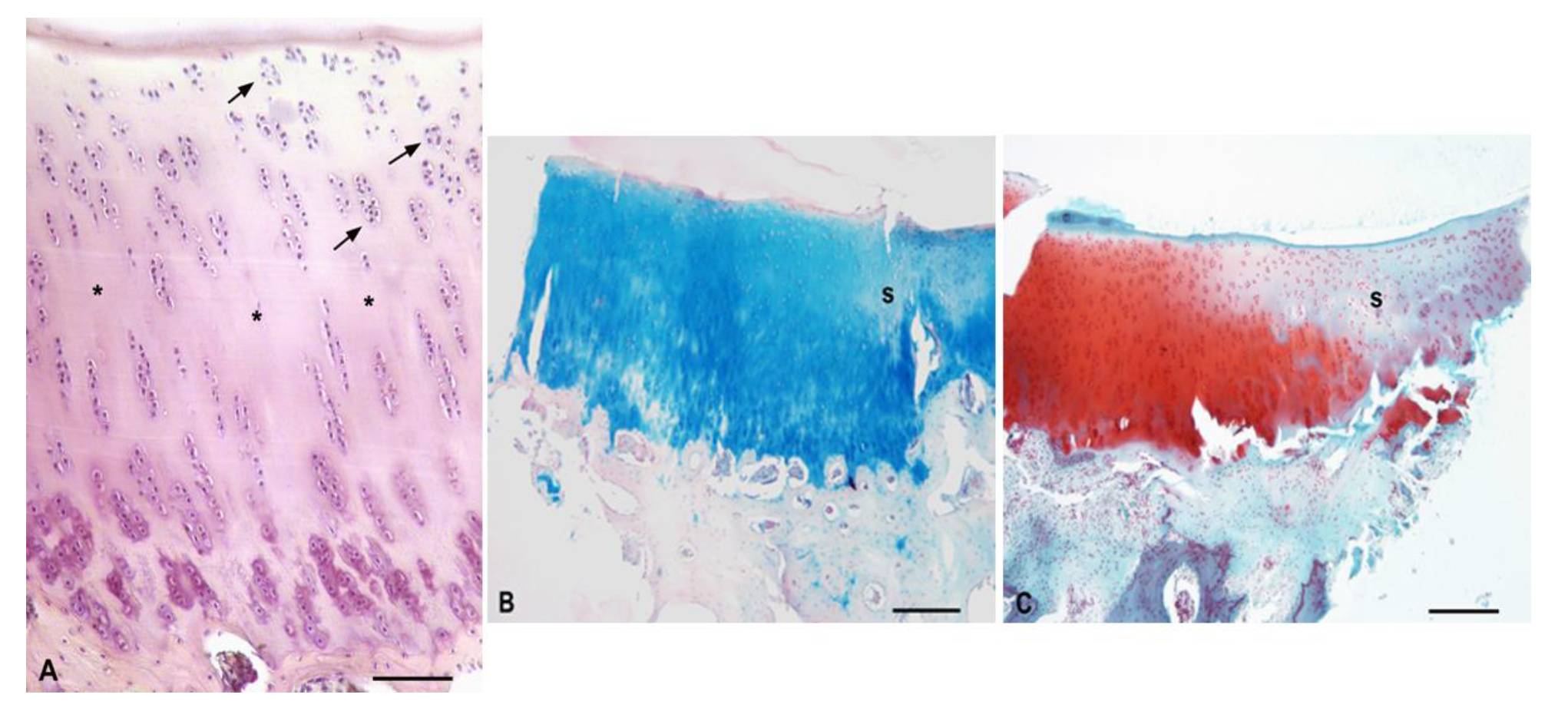
3.5. Histological Evaluation of Repaired Cartilage Defects
3.5.1. Experimental Sheep 1
3.5.2. Experimental Sheep 2
3.5.3. Experimental Sheep 3
3.5.4. Experimental Sheep 4
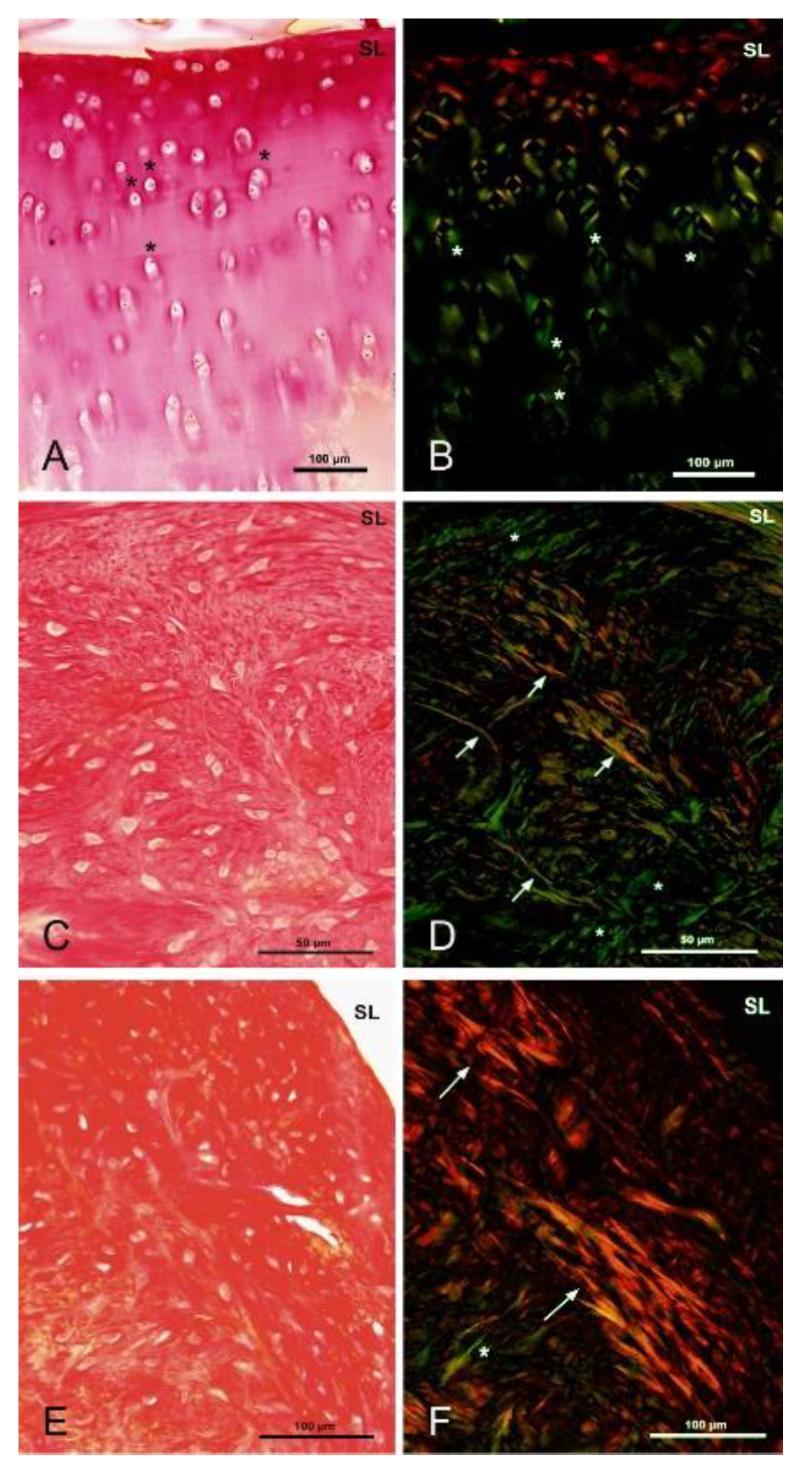
3.5.5. Polarized Microscopy Evaluation of Collagen
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ross, M.H.; Pawlina, W. Histology: A Text and Atlas, 6th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Baltimore, MA, USA, 2011; pp. 198–207. [Google Scholar]
- Karuppal, R. Current concepts in the articular cartilage repair and regeneration. J. Orthop. 2017, 14, A1–A3. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, G. New perspectives for articular cartilage repair treatment through tissue engineering: A contemporary review. World J. Orthop. 2014, 5, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulet, B. Models to define the stages of articular cartilage degradation in osteoarthritis development. Int. J. Exp. Pathol. 2017, 98, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Music, E.; Futrega, K.; Doran, M. Sheep as a model for evaluating mesenchymal stem/stromal cell (MSC)-based chondral defect repair. Osteoarthr. Cartil. 2018, 26, 730–740. [Google Scholar] [CrossRef] [Green Version]
- Neidlin, M.; Chantzi, E.; Macheras, G.; Gustafsson, M.G.; Alexopoulos, L.G. An ex vivo tissue model of cartilage degradation suggests that cartilage state can be determined from secreted key protein patterns. PLoS ONE 2019, 14, e0224231. [Google Scholar] [CrossRef] [Green Version]
- Berenbaum, F.; Wallace, I.J.; Lieberman, D.E.; Felson, D.T. Modern-day environmental factors in the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2018, 14, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Bortoluzzi, A.; Furini, F.; Scirè, C.A. Osteoarthritis and its management—Epidemiology, nutritional aspects and environmental factors. Autoimmun. Rev. 2018, 17, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Medvedeva, E.V.; Grebenik, E.A.; Gornostaeva, S.N.; Telpuhov, V.I.; Lychagin, A.V.; Timashev, P.S.; Chagin, A.S. Repair of Damaged Articular Cartilage: Current Approaches and Future Directions. Int. J. Mol. Sci. 2018, 19, 2366. [Google Scholar] [CrossRef] [Green Version]
- Redman, S.N.; Oldfield, S.F.; Archer, C.W. Current strategies for articular cartilage repair. Eur. Cells Mater. 2005, 9, 23–32. [Google Scholar] [CrossRef]
- Chu, C.R.; Szczodry, M.; Bruno, S. Animal Models for Cartilage Regeneration and Repair. Tissue Eng. Part B Rev. 2010, 16, 105–115. [Google Scholar] [CrossRef]
- Dias, I.R.; Viegas, C.A.; Carvalho, P.P. Large Animal Models for Osteochondral Regeneration. Tissue Eng. 2018, 1059, 441–501. [Google Scholar] [CrossRef]
- Hoemann, C.D.; Hurtig, M.; Rossomacha, E.; Sun, J.; Chevrier, A.; Shive, M.S.; Buschmann, M.D. Chitosan-Glycerol Phosphate/Blood Implants Improve Hyaline Cartilage Repair in Ovine Microfracture Defects. J. Bone Jt. Surg. Am. Vol. 2005, 87, 2671–2686. [Google Scholar] [CrossRef]
- Hao, T.; Wen, N.; Cao, J.-K.; Wang, H.-B.; Lü, S.-H.; Liu, T.; Lin, Q.-X.; Duan, C.-M.; Wang, C.-Y. The support of matrix accumulation and the promotion of sheep articular cartilage defects repair in vivo by chitosan hydrogels. Osteoarthr. Cartil. 2010, 18, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Zhu, C.; Wu, Q.; Wang, F.; Zhang, X.; Chen, F.; Liu, X.; Yang, Q.; Zhu, L. Animal Models Used for Testing Hydrogels in Cartilage Regeneration. Curr. Stem Cell Res. Ther. 2018, 13, 517–525. [Google Scholar] [CrossRef]
- Kim, I.-Y.; Seo, S.-J.; Moon, H.-S.; Yoo, M.-K.; Park, I.-Y.; Kim, B.-C.; Cho, C.-S. Chitosan and its derivatives for tissue engineering applications. Biotechnol. Adv. 2008, 26, 1–21. [Google Scholar] [CrossRef]
- Rogina, A.; Pušić, M.; Štefan, L.; Ivković, A.; Urlić, I.; Ivanković, M.; Ivanković, H. Characterization of Chitosan-Based Scaffolds Seeded with Sheep Nasal Chondrocytes for Cartilage Tissue Engineering. Ann. Biomed. Eng. 2021, 1–15. [Google Scholar] [CrossRef]
- Victor, R.D.S.; Santos, A.M.D.C.; De Sousa, B.V.; Neves, G.D.A.; Santana, L.N.D.L.; Menezes, R.R. A Review on Chitosan’s Uses as Biomaterial: Tissue Engineering, Drug Delivery Systems and Cancer Treatment. Materials 2020, 13, 4995. [Google Scholar] [CrossRef]
- Concha, M.; Vidal, A.; Giacaman, A.; Ojeda, J.; Pavicic, F.; Oyarzun-Ampuero, F.A.; Torres, C.; Cabrera, M.; Moreno-Villoslada, I.; Orellana, S.L. Aerogels made of chitosan and chondroitin sulfate at high degree of neutralization: Biological properties toward wound healing. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 2464–2471. [Google Scholar] [CrossRef]
- Oryan, A.; Sahvieh, S. Effectiveness of chitosan scaffold in skin, bone and cartilage healing. Int. J. Biol. Macromol. 2017, 104, 1003–1011. [Google Scholar] [CrossRef]
- Oprenyeszk, F.; Sanchez, C.; Dubuc, J.-É.; Maquet, V.; Henrist, C.; Compère, P.; Henrotin, Y. Chitosan Enriched Three-Dimensional Matrix Reduces Inflammatory and Catabolic Mediators Production by Human Chondrocytes. PLoS ONE 2015, 10, e0128362. [Google Scholar] [CrossRef] [Green Version]
- Comblain, F.; Rocasalbas, G.; Gauthier, S.; Henrotin, Y. Chitosan: A promising polymer for cartilage repair and viscosupplementation. Bio Med. Mater. Eng. 2017, 28, S209–S215. [Google Scholar] [CrossRef]
- Islam, M.; Shahruzzaman, M.; Biswas, S.; Sakib, N.; Rashid, T.U. Chitosan based bioactive materials in tissue engineering applications-A review. Bioact. Mater. 2020, 5, 164–183. [Google Scholar] [CrossRef]
- Hill, R.G. Biomedical polymers. In Biomaterials, Artificial Organs and Tissue Engineering; Elsevier: Amsterdam, The Netherlands, 2005; pp. 97–106. [Google Scholar]
- Dariš, B.; Knez, Ž. Poly(3-hydroxybutyrate): Promising biomaterial for bone tissue engineering. Acta Pharm. 2020, 70, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giretova, M.; Medvecky, L.; Petrovova, E.; Cizkova, D.; Danko, J.; Mudronova, D.; Slovinska, L.; Bures, R. Polyhydroxybutyrate/Chitosan 3D Scaffolds Promote In Vitro and In Vivo Chondrogenesis. Appl. Biochem. Biotechnol. 2019, 189, 556–575. [Google Scholar] [CrossRef] [PubMed]
- Kok, A.C.; van Bergen, C.J.A.; Tuijthof, G.J.M.; Klinkenbijl, M.N.; van Noorden, C.J.F.; van Dijk, C.N.; Kerkhoffs, G.M.M.J. Macroscopic ICRS Poorly Correlates with O’Driscoll Histological Cartilage Repair Assessment in a Goat Model. Clin. Res. Foot Ankle 2015, 3, 1–7. [Google Scholar] [CrossRef]
- Moojen, D.; Saris, D.; Yang, K.A.; Dhert, W.; Verbout, A. The Correlation and Reproducibility of Histological Scoring Systems in Cartilage Repair. Tissue Eng. 2002, 8, 627–634. [Google Scholar] [CrossRef]
- Orth, P.; Madry, H. Complex and elementary histological scoring systems for articular cartilage repair. Histol. Histopathol. 2015, 30, 911–919. [Google Scholar]
- Medvecky, L.; Giretova, M.; Stulajterova, R. Properties and in vitro characterization of polyhydroxybutyrate–chitosan scaffolds prepared by modified precipitation method. J. Mater. Sci. Mater. Electron. 2014, 25, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Giretova, M.; Medvecky, L.; Stulajterova, R.; Sopcak, T.; Briancin, J.; Tatarkova, M. Effect of enzymatic degradation of chitosan in polyhydroxybutyrate/chitosan/calcium phosphate composites on in vitro osteoblast response. J. Mater. Sci. Mater. Electron. 2016, 27, 181. [Google Scholar] [CrossRef] [PubMed]
- Tothova, C.; Mihajlovicova, X.; Novotny, J.; Nagy, O.; Giretova, M.; Kresakova, L.; Tomco, M.; Zert, Z.; Vilhanova, Z.; Varga, M.; et al. The Serum Protein Profile and Acute Phase Proteins in the Postoperative Period in Sheep after Induced Articular Cartilage Defect. Materials 2019, 12, 142. [Google Scholar] [CrossRef] [Green Version]
- Junqueira, L.C.U.; Bignolas, G.; Brentani, R.R. Picrosirius staining plus polarization microscopy, a specific method for collagen detection in tissue sections. J. Mol. Histol. 1979, 11, 447–455. [Google Scholar] [CrossRef]
- Rutgers, M.; van Pelt, M.; Dhert, W.; Creemers, L.; Saris, D. Evaluation of histological scoring systems for tissue-engineered, repaired and osteoarthritic cartilage. Osteoarthr. Cartil. 2010, 18, 12–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, M.J.; Houlton, J.E.F.; Adams, S.B.; Rushton, N. The Surgical Anatomy of the Stifle Joint in Sheep. Veter Surg. 1998, 27, 596–605. [Google Scholar] [CrossRef] [PubMed]
- McIlwrith, C.W.; Frisbie, D.D.; Kawcak, C.E.; van Weeren, R. Joint Disease. In The Horse, 2nd ed.; Elsevier: St. Louis, MO, USA, 2016; pp. 2–3. [Google Scholar]
- Armiento, A.R.; Alini, M.; Stoddart, M.J. Articular fibrocartilage—Why does hyaline cartilage fail to repair? Adv. Drug Deliv. Rev. 2019, 146, 289–305. [Google Scholar] [CrossRef] [PubMed]
- Gottardi, R.; Hansen, U.; Raiteri, R.; Loparic, M.; Düggelin, M.; Mathys, D.; Friederich, N.F.; Bruckner, P.; Stolz, M. Supramolecular Organization of Collagen Fibrils in Healthy and Osteoarthritic Human Knee and Hip Joint Cartilage. PLoS ONE 2016, 11, e0163552. [Google Scholar] [CrossRef]
- Guilak, F.; Nims, R.J.; Dicks, A.; Wu, C.-L.; Meulenbelt, I. Osteoarthritis as a disease of the cartilage pericellular matrix. Matrix Biol. 2018, 71–72, 40–50. [Google Scholar] [CrossRef]
- Ravanetti, F.; Galli, C.; Manfredi, E.; Cantoni, A.M.; Scarpa, E.; Macaluso, G.M.; Cacchioli, A. Chitosan-based scaffold modified with D-(+) raffinose for cartilage repair: An in vivo study. J. Negat. Results Biomed. 2015, 14, 2. [Google Scholar] [CrossRef] [Green Version]
- Roffi, A.; Kon, E.; Perdisa, F.; Fini, M.; Di Martino, A.; Parrilli, A.; Salamanna, F.; Sandri, M.; Sartori, M.; Sprio, S.; et al. A Composite Chitosan-Reinforced Scaffold Fails to Provide Osteochondral Regeneration. Int. J. Mol. Sci. 2019, 20, 2227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoemann, C.D.; Guzmán-Morales, J.; Picard, G.; Chen, G.; Veilleux, D.; Chevrier, A.; Sim, S.; Garon, M.; Quenneville, E.; Lafantaisie-Favreau, C.-H.; et al. Guided bone marrow stimulation for articular cartilage repair through a freeze-dried chitosan microparticle approach. Materials 2020, 9, 100609. [Google Scholar] [CrossRef]
- Gupta, A.; Bhat, S.; Jagdale, P.R.; Chaudhari, B.P.; Lidgren, L.; Gupta, K.C.; Kumar, A. Evaluation of Three-Dimensional Chitosan-Agarose-Gelatin Cryogel Scaffold for the Repair of Subchondral Cartilage Defects: AnIn VivoStudy in a Rabbit Model. Tissue Eng. Part A 2014, 20, 3101–3111. [Google Scholar] [CrossRef] [Green Version]
- Petrovova, E.; Giretova, M.; Kvasilova, A.; Benada, O.; Danko, J.; Medvecky, L.; Sedmera, D. Preclinical alternative model for analysis of porous scaffold biocompatibility in bone tissue engineering. ALTEX 2019, 36, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.D.; Hurtig, M.B.; Quenneville, E.; Rivard, G.-É.; Hoemann, C.D. Effect of a Rapidly Degrading Presolidified 10 kDa Chitosan/Blood Implant and Subchondral Marrow Stimulation Surgical Approach on Cartilage Resurfacing in a Sheep Model. Cartilage 2017, 8, 417–431. [Google Scholar] [CrossRef]
- Ruediger, T.; Horbert, V.; Reuther, A.; Kalla, P.K.; Burgkart, R.H.; Walther, M.; Kinne, R.W.; Mika, J. Thickness of the Stifle Joint Articular Cartilage in Different Large Animal Models of Cartilage Repair and Regeneration. Cartilage 2020, 7, 126–147. [Google Scholar] [CrossRef]
- Ahern, B.; Parvizi, J.; Boston, R.; Schaer, T. Preclinical animal models in single site cartilage defect testing: A systematic review. Osteoarthr. Cartil. 2009, 17, 705–713. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Hu, J.; Athanasiou, K.A. The Role of Tissue Engineering in Articular Cartilage Repair and Regeneration. Crit. Rev. Biomed. Eng. 2009, 37, 1–57. [Google Scholar] [CrossRef] [PubMed]
- Vyas, C.; Mishbak, H.; Cooper, G.; Peach, C.; Pereira, R.F.; Bartolo, P. Biological perspectives and current biofabrication strategies in osteochondral tissue engineering. Biomanuf. Rev. 2020, 5, 1–24. [Google Scholar] [CrossRef]
- Matsiko, A.; Levingstone, T.J.; O’Brien, F.J. Advanced Strategies for Articular Cartilage Defect Repair. Materials 2013, 6, 637–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldracher, M.; Orth, P.; Cucchiarini, M.; Pape, D.; Madry, H. Small Subchondral Drill Holes Improve Marrow Stimulation of Articular Cartilage Defects. Am. J. Sports Med. 2014, 42, 2741–2750. [Google Scholar] [CrossRef]
- Pot, M.W.; Gonzales, V.K.; Buma, P.; IntHout, J.; Van Kuppevelt, T.H.; De Vries, R.B.; Daamen, W.F. Improved cartilage regeneration by implantation of acellular biomaterials after bone marrow stimulation: A systematic review and meta-analysis of animal studies. PeerJ 2016, 4, e2243. [Google Scholar] [CrossRef]
- Fox, A.J.S.; Bedi, A.; Rodeo, S.A. The Basic Science of Articular Cartilage: Structure, Composition, and Function. Sports Health A Multidiscip. Approach 2009, 1, 461–468. [Google Scholar] [CrossRef]
- Mohan, N.; Mohanan, P.; Sabareeswaran, A.; Nair, P. Chitosan-hyaluronic acid hydrogel for cartilage repair. Int. J. Biol. Macromol. 2017, 104, 1936–1945. [Google Scholar] [CrossRef] [PubMed]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Animals | Defects Location | Scaffold Implantation |
|---|---|---|
| Experimental sheep 1 | left trochlea | + |
| left condyle | + | |
| Experimental sheep 2 | left trochlea | + |
| left condyle | + | |
| Experimental sheep 3 | left trochlea | + |
| left condyle | + | |
| Experimental sheep 4 | left trochlea | + |
| left condyle | + | |
| Experimental sheep 5 | left trochlea | - |
| left condyle | - | |
| Experimental sheep 6 | left trochlea | - |
| left condyle | - |
| Sample | Average T | Reference Average | Percentage Difference (%) |
|---|---|---|---|
| Experimental sheep 1 | 28,559.66 | 28,659.53 | 0.35 |
| Experimental sheep 2 | 38,320.75 | 39,369.86 | 2.67 |
| Experimental sheep 3 | 29,388.88 | 29,407.09 | 0.06 |
| Experimental sheep 4 | 34,143.07 | 35,803.56 | 4.64 |
| Parameters | Untreated Sheep 1 | Untreated Sheep 2 | Experimental Sheep 1 | Experimental Sheep 2 | Experimental Sheep 3 | Experimental Sheep 4 |
|---|---|---|---|---|---|---|
| Degenerative changes in adjacent cartilage | 1.67 ± 0.58 | 2.00 ± 0.00 | 1.20 ± 0.45 | 2.00 ± 0.00 | 2.00 ± 0.71 | 2.75 ± 0.50 |
| Chondrocyte clustering | 1.00 ± 0.00 | 1.50 ± 0.58 | 0.60 ± 0.55 | 1.00 ± 0.00 | 2.00 ± 0.00 | 1.50 ± 0.60 |
| Hypocellularity | 2.67 ± 0.58 | 3.00 ± 0.00 | 2.20 ± 0.45 | 3.00 ± 0.00 | 3.00 ± 0.00 | 2.50 ± 0.60 |
| Bonding to the adjacent cartilage | 1.00 ± 0.00 | 1.00 ± 0.00 | 1.00 ± 0.00 | 1.00 ± 0.00 | 1.00 ± 0.00 | 1.00 ± 0.00 |
| Thickness of cartilage | 1.00 ± 0.00 | 1.00 ± 0.00 | 1.20 ± 0.45 | 2.00 ± 0.00 | 1.40 ± 0.55 | 1.00 ± 0.00 |
| Structural integrity | 2.00 ± 0.00 | 2.00 ± 0.00 | 1.80 ± 0.45 | 2.00 ± 0.00 | 1.40 ± 0.89 | 0.75 ± 0.96 |
| Surface regularity | 1.67 ± 1.15 | 3.00 ± 0.00 | 1.20 ± 0.45 | 3.00 ± 0.00 | 2.00 ± 0.70 | 2.75 ± 0.50 |
| Safranin-O staining of the matrix | 2.00 ± 0.00 | 2.00 ± 0.00 | 2.00 ± 0.00 | 1.60 ± 0.55 | 2.00 ± 0.00 | 3.00 ± 0.00 |
| Cell morphology | 0.00 ± 0.00 | 0.00 ± 0.00 | 4.00 ± 0.00 | 4.00 ± 0.00 | 3.20 ± 1.79 | 0.00 ± 0.00 |
| Total average score | 13.00 ± 2.00 | 15.50 ± 0.58 | 15.20 ± 1.48 | 19.60 ± 0.55 | 18.20 ± 3.63 | 15.50 ± 1.29 |
| Parameters | Untreated Sheep 1 | Untreated Sheep 2 | Experimental Sheep 1 | Experimental Sheep 2 | Experimental Sheep 3 | Experimental Sheep 4 |
|---|---|---|---|---|---|---|
| Cell morphology | 1.33 ± 0.52 | 1.80 ± 0.49 | 1.00 ± 0.00 | 0.00 ± 0.00 | 1.00 ± 0.00 | 1.40 ± 0.55 |
| Staining of the matrix | 1.17 ± 0.41 | 1.00 ± 0.00 | 1.00 ± 0.00 | 0.6 ± 0.55 | 0.20 ± 0.45 | 0.00 ± 0.00 |
| Reconstitution of the osteochondral junction | 0.83 ± 0.41 | 0.29 ± 0.49 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 |
| Filling of the defect | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.80 ± 0.84 | 0.00 ± 0.00 | 0.40 ± 0.55 | 0.00 ± 0.00 |
| Total average score | 3.33 ± 0.82 | 3.00 ± 0.58 | 2.80 ± 0.75 | 0.60 ± 0.55 | 1.20 ± 0.45 | 1.40 ± 0.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrovova, E.; Tomco, M.; Holovska, K.; Danko, J.; Kresakova, L.; Vdoviakova, K.; Simaiova, V.; Kolvek, F.; Hornakova, P.; Toth, T.; et al. PHB/CHIT Scaffold as a Promising Biopolymer in the Treatment of Osteochondral Defects—An Experimental Animal Study. Polymers 2021, 13, 1232. https://doi.org/10.3390/polym13081232
Petrovova E, Tomco M, Holovska K, Danko J, Kresakova L, Vdoviakova K, Simaiova V, Kolvek F, Hornakova P, Toth T, et al. PHB/CHIT Scaffold as a Promising Biopolymer in the Treatment of Osteochondral Defects—An Experimental Animal Study. Polymers. 2021; 13(8):1232. https://doi.org/10.3390/polym13081232
Chicago/Turabian StylePetrovova, Eva, Marek Tomco, Katarina Holovska, Jan Danko, Lenka Kresakova, Katarina Vdoviakova, Veronika Simaiova, Filip Kolvek, Petra Hornakova, Teodor Toth, and et al. 2021. "PHB/CHIT Scaffold as a Promising Biopolymer in the Treatment of Osteochondral Defects—An Experimental Animal Study" Polymers 13, no. 8: 1232. https://doi.org/10.3390/polym13081232