
Exercise Training Combined with Calanus Oil Supplementation Improves the Central Cardiodynamic Function in Older Women

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Study Design
2.2. Clinical Examinations
2.3. Bicycle Ergometry with PhysioFlow Hemodynamic Testing
2.4. Plasma Analysis
2.5. Statistics
3. Results
3.1. Exercise Training Combined with Calanus Oil Supplementation Affects the Body Composition
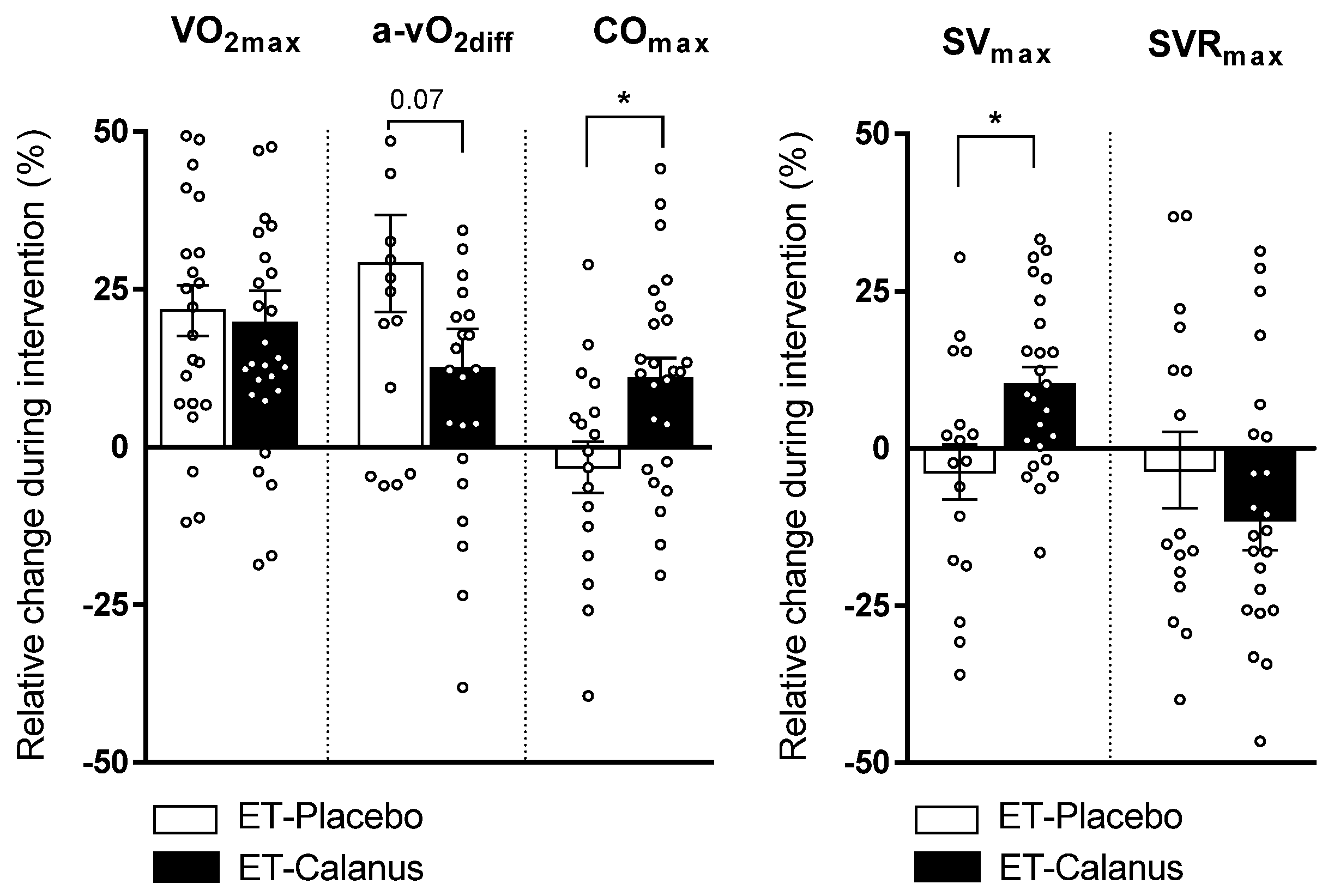
3.2. Exercise Training Combined with Calanus Supplementation Affects the Central Cardiorespiratory Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990S–991S. [Google Scholar] [CrossRef] [Green Version]
- Zamboni, M.; Rossi, A.P.; Fantin, F.; Zamboni, G.; Chirumbolo, S.; Zoico, E.; Mazzali, G. Adipose tissue, diet and aging. Mech. Ageing Dev. 2014, 136–137, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Mei, Y.-X.; Wu, H.; Zhang, H.-Y.; Hou, J.; Zhang, Z.-X.; Liao, W.; Liu, X.-T.; Sang, S.-X.; Mao, Z.-X.; Yang, D.-B.; et al. Health-related quality of life and its related factors in coronary heart disease patients: Results from the Henan Rural Cohort study. Sci. Rep. 2021, 11, 5011. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Sui, X.; Lobelo, F.; Morrow, J.R., Jr.; Jackson, A.W.; Sjostrom, M.; Blair, S.N. Association between muscular strength and mortality in men: Prospective cohort study. BMJ 2008, 337, a439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, Y.; Tanaka, Y.; Sato, F.; Choi, J.B.; Watada, H.; Niwa, M.; Kinoshita, J.; Ooka, A.; Kumashiro, N.; Igarashi, Y.; et al. Effects of diet and exercise on muscle and liver intracellular lipid contents and insulin sensitivity in type 2 diabetic patients. J. Clin. Endocrinol. Metab. 2005, 90, 3191–3196. [Google Scholar] [CrossRef] [Green Version]
- Way, K.L.; Hackett, D.A.; Baker, M.K.; Johnson, N.A. The Effect of Regular Exercise on Insulin Sensitivity in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Metab. J. 2016, 40, 253–271. [Google Scholar] [CrossRef]
- Williams, M.A.; Stewart, K.J. Impact of strength and resistance training on cardiovascular disease risk factors and outcomes in older adults. Clin. Geriatr. Med. 2009, 25, 703–714. [Google Scholar] [CrossRef]
- Lavie, C.J.; Arena, R.; Swift, D.L.; Johannsen, N.M.; Sui, X.; Lee, D.C.; Earnest, C.P.; Church, T.S.; O’Keefe, J.H.; Milani, R.V.; et al. Exercise and the cardiovascular system: Clinical science and cardiovascular outcomes. Circ. Res. 2015, 117, 207–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.C.; Sui, X.; Artero, E.G.; Lee, I.M.; Church, T.S.; McAuley, P.A.; Stanford, F.C.; Kohl, H.W., 3rd; Blair, S.N. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: The Aerobics Center Longitudinal Study. Circulation 2011, 124, 2483–2490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marik, P.E.; Varon, J. Omega-3 dietary supplements and the risk of cardiovascular events: A systematic review. Clin. Cardiol. 2009, 32, 365–372. [Google Scholar] [CrossRef]
- Rizos, E.C.; Ntzani, E.E.; Bika, E.; Kostapanos, M.S.; Elisaf, M.S. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: A systematic review and meta-analysis. JAMA 2012, 308, 1024–1033. [Google Scholar] [CrossRef]
- Walser, B.; Stebbins, C.L. Omega-3 fatty acid supplementation enhances stroke volume and cardiac output during dynamic exercise. Eur. J. Appl. Physiol. 2008, 104, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Capó, X.; Martorell, M.; Sureda, A.; Llompart, I.; Tur, J.A.; Pons, A. Diet supplementation with DHA-enriched food in football players during training season enhances the mitochondrial antioxidant capabilities in blood mononuclear cells. Eur. J. Nutr. 2015, 54, 35–49. [Google Scholar] [CrossRef]
- Toko, H.; Morita, H.; Katakura, M.; Hashimoto, M.; Ko, T.; Bujo, S.; Adachi, Y.; Ueda, K.; Murakami, H.; Ishizuka, M.; et al. Omega-3 fatty acid prevents the development of heart failure by changing fatty acid composition in the heart. Sci. Rep. 2020, 10, 15553. [Google Scholar] [CrossRef] [PubMed]
- Hoper, A.C.; Salma, W.; Khalid, A.M.; Hafstad, A.D.; Sollie, S.J.; Raa, J.; Larsen, T.S.; Aasum, E. Oil from the marine zooplankton Calanus finmarchicus improves the cardiometabolic phenotype of diet-induced obese mice. Br. J. Nutr. 2013, 110, 2186–2193. [Google Scholar] [CrossRef] [Green Version]
- Jansen, K.M.; Moreno, S.; Garcia-Roves, P.M.; Larsen, T.S. Dietary Calanus oil recovers metabolic flexibility and rescues postischemic cardiac function in obese female mice. Am. J. Physiol. Heart Circ. Physiol. 2019, 317, H290–H299. [Google Scholar] [CrossRef]
- Cook, C.M.; Larsen, T.S.; Derrig, L.D.; Kelly, K.M.; Tande, K.S. Wax Ester Rich Oil From The Marine Crustacean, Calanus finmarchicus, is a Bioavailable Source of EPA and DHA for Human Consumption. Lipids 2016, 51, 1137–1144. [Google Scholar] [CrossRef]
- Bergvik, M.; Leiknes, O.; Altin, D.; Dahl, K.R.; Olsen, Y. Dynamics of the lipid content and biomass of Calanus finmarchicus (copepodite V) in a Norwegian Fjord. Lipids 2012, 47, 881–895. [Google Scholar] [CrossRef]
- Schots, P.C.; Pedersen, A.M.; Eilertsen, K.E.; Olsen, R.L.; Larsen, T.S. Possible Health Effects of a Wax Ester Rich Marine Oil. Front Pharm. 2020, 11, 961. [Google Scholar] [CrossRef] [PubMed]
- Naguib, Y.M. Antioxidant activities of astaxanthin and related carotenoids. J. Agric. Food Chem. 2000, 48, 1150–1154. [Google Scholar] [CrossRef] [PubMed]
- Cizkova, T.; Stepan, M.; Dadova, K.; Ondrujova, B.; Sontakova, L.; Krauzova, E.; Matous, M.; Koc, M.; Gojda, J.; Kracmerova, J.; et al. Exercise Training Reduces Inflammation of Adipose Tissue in the Elderly: Cross-Sectional and Randomized Interventional Trial. J. Clin. Endocrinol. Metab. 2020, 105, e4510–e4526. [Google Scholar] [CrossRef] [PubMed]
- Daďová, K.; Petr, M.; Šteffl, M.; Sontáková, L.; Chlumský, M.; Matouš, M.; Štich, V.; Štěpán, M.; Šiklová, M. Effect of Calanus Oil Supplementation and 16 Week Exercise Program on Selected Fitness Parameters in Older Women. Nutrients 2020, 12, 481. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D.; Rimm, E.B. Fish intake, contaminants, and human health: Evaluating the risks and the benefits. JAMA 2006, 296, 1885–1899. [Google Scholar] [CrossRef] [Green Version]
- Fielding, B.A. Omega-3 index as a prognosis tool in cardiovascular disease. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 360–365. [Google Scholar] [CrossRef] [Green Version]
- Brezinova, M.; Cajka, T.; Oseeva, M.; Stepan, M.; Dadova, K.; Rossmeislova, L.; Matous, M.; Siklova, M.; Rossmeisl, M.; Kuda, O. Exercise training induces insulin-sensitizing PAHSAs in adipose tissue of elderly women. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2020, 1865, 158576. [Google Scholar] [CrossRef]
- Stults-Kolehmainen, M.A.; Stanforth, P.R.; Bartholomew, J.B.; Lu, T.; Abolt, C.J.; Sinha, R. DXA estimates of fat in abdominal, trunk and hip regions varies by ethnicity in men. Nutr. Diabetes 2013, 3, e64. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Represas, A.; Mourot, L. Stroke volume and cardiac output measurement in cardiac patients during a rehabilitation program: Comparison between tonometry, impedancemetry and echocardiography. Int. J. Cardiovasc. Imaging 2020, 36, 447–455. [Google Scholar] [CrossRef]
- Louvaris, Z.; Spetsioti, S.; Andrianopoulos, V.; Chynkiamis, N.; Habazettl, H.; Wagner, H.; Zakynthinos, S.; Wagner, P.D.; Vogiatzis, I. Cardiac output measurement during exercise in COPD: A comparison of dye dilution and impedance cardiography. Clin. Respir. J. 2019, 13, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Siebenmann, C.; Rasmussen, P.; Sorensen, H.; Zaar, M.; Hvidtfeldt, M.; Pichon, A.; Secher, N.H.; Lundby, C. Cardiac output during exercise: A comparison of four methods. Scand. J. Med. Sci. Sports 2015, 25, e20–e27. [Google Scholar] [CrossRef] [PubMed]
- Murias, J.M.; Kowalchuk, J.M.; Paterson, D.H. Mechanisms for increases in V O2max with endurance training in older and young women. Med. Sci. Sports Exerc. 2010, 42, 1891–1898. [Google Scholar] [CrossRef]
- Spina, R.J. Cardiovascular adaptations to endurance exercise training in older men and women. Exerc. Sport Sci. Rev. 1999, 27, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Storen, O.; Helgerud, J.; Saebo, M.; Stoa, E.M.; Bratland-Sanda, S.; Unhjem, R.J.; Hoff, J.; Wang, E. The Effect of Age on the V O2max Response to High-Intensity Interval Training. Med. Sci. Sports Exerc. 2017, 49, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Salma, W.; Franekova, V.; Lund, T.; Hoper, A.; Ludvigsen, S.; Lund, J.; Aasum, E.; Ytrehus, K.; Belke, D.D.; Larsen, T.S. Dietary Calanus oil antagonizes angiotensin II-induced hypertension and tissue wasting in diet-induced obese mice. Prostaglandins Leukot Essent Fat. Acids 2016, 108, 13–21. [Google Scholar] [CrossRef]
- Bloomer, R.J.; Larson, D.E.; Fisher-Wellman, K.H.; Galpin, A.J.; Schilling, B.K. Effect of eicosapentaenoic and docosahexaenoic acid on resting and exercise-induced inflammatory and oxidative stress biomarkers: A randomized, placebo controlled, cross-over study. Lipids Health Dis. 2009, 8, 36. [Google Scholar] [CrossRef] [Green Version]
- Bouwens, M.; van de Rest, O.; Dellschaft, N.; Bromhaar, M.G.; de Groot, L.C.; Geleijnse, J.M.; Muller, M.; Afman, L.A. Fish-oil supplementation induces antiinflammatory gene expression profiles in human blood mononuclear cells. Am. J. Clin. Nutr. 2009, 90, 415–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rababa’h, A.M.; Guillory, A.N.; Mustafa, R.; Hijjawi, T. Oxidative Stress and Cardiac Remodeling: An Updated Edge. Curr Cardiol Rev 2018, 14, 53–59. [Google Scholar] [CrossRef]
- Fulghum, K.; Hill, B.G. Metabolic Mechanisms of Exercise-Induced Cardiac Remodeling. Front. Cardiovasc. Med. 2018, 5, 127. [Google Scholar] [CrossRef] [Green Version]
- Antuna-Puente, B.; Feve, B.; Fellahi, S.; Bastard, J.P. Adipokines: The missing link between insulin resistance and obesity. Diabetes Metab. 2008, 34, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Kolwicz, S.C., Jr. An “Exercise” in Cardiac Metabolism. Front. Cardiovasc. Med. 2018, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Sloan, C.; Tuinei, J.; Nemetz, K.; Frandsen, J.; Soto, J.; Wride, N.; Sempokuya, T.; Alegria, L.; Bugger, H.; Abel, E.D. Central leptin signaling is required to normalize myocardial fatty acid oxidation rates in caloric-restricted ob/ob mice. Diabetes 2011, 60, 1424–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Wang, M.Y.; Kakuma, T.; Wang, Z.W.; Babcock, E.; McCorkle, K.; Higa, M.; Zhou, Y.T.; Unger, R.H. Liporegulation in diet-induced obesity. The antisteatotic role of hyperleptinemia. J. Biol. Chem. 2001, 276, 5629–5635. [Google Scholar] [CrossRef] [Green Version]
- Wasserfurth, P.; Nebl, J.; Schuchardt, J.P.; Muller, M.; Bosslau, T.K.; Kruger, K.; Hahn, A. Effects of Exercise Combined with a Healthy Diet or Calanus finmarchicus Oil Supplementation on Body Composition and Metabolic Markers-A Pilot Study. Nutrients 2020, 12, 2139. [Google Scholar] [CrossRef] [PubMed]
- McGlory, C.; Calder, P.C.; Nunes, E.A. The Influence of Omega-3 Fatty Acids on Skeletal Muscle Protein Turnover in Health, Disuse, and Disease. Front. Nutr. 2019, 6, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzawa, Y.; Funahashi, T.; Nakamura, T. The concept of metabolic syndrome: Contribution of visceral fat accumulation and its molecular mechanism. J. Atheroscler. Thromb. 2011, 18, 629–639. [Google Scholar] [CrossRef] [Green Version]
- Cornish, S.M.; Myrie, S.B.; Bugera, E.M.; Chase, J.E.; Turczyn, D.; Pinder, M. Omega-3 supplementation with resistance training does not improve body composition or lower biomarkers of inflammation more so than resistance training alone in older men. Nutr. Res. 2018, 60, 87–95. [Google Scholar] [CrossRef]
- Rodacki, C.L.; Rodacki, A.L.; Pereira, G.; Naliwaiko, K.; Coelho, I.; Pequito, D.; Fernandes, L.C. Fish-oil supplementation enhances the effects of strength training in elderly women. Am. J. Clin. Nutr. 2012, 95, 428–436. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Fatty Acid | Calanus Oil | Sunflower Oil | |
|---|---|---|---|
| % of Total Fatty Acids | |||
| Myristic acid | 14:0 | 15.37 | nd |
| Palmitic acid | 16:0 | 12.84 | 6.3 |
| Stearic acid | 18:0 | 0.85 | 4.6 |
| Arachidic acid | 20:0 | 0.10 | 0.5 |
| Palmitoleic acid | 16:1 n-7 | 3.80 | 0.3 |
| Oleic acid | 18:1 n-9 | 4.32 | 26.7 |
| Gondoic acid | 20:1 n-9 | 3.63 | nd |
| Gadoleic acid | 20:1 n-11 | 3.90 | nd |
| Cetoleic acid | 22:1 n-11 | 5.06 | nd |
| Nervonic acid | 24:1 n-9 | 0.58 | nd |
| Linoleic acid | 18:2 n-6 | 1.65 | 61.1 |
| Linolenic acid | 18:3 n-3 | 4.38 | 0.3 |
| Stearidonic acid | 18:4 n-3 | 20.50 | nd |
| Arachidonic acid | 20:4 n-3 | 0.38 | nd |
| Eicosapentaenic acid | 20:5 n-3 | 10.98 | nd |
| Docosahexaenoic acid | 22:6 n-3 | 9.26 | nd |
| Sum of fatty acids | |||
| SFA (g/100g oil) | 14.7 | 12.3 | |
| MUFA (g/100g oil) | 14.0 | 28.7 | |
| PUFA (g/100g oil) | 20.4 | 59.0 | |
| Fatty alcohol | 39.0 | nd | |
| ET-Placebo | ET-Calanus | Two-Way ANOVA p-Value | |||||
|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Time | Group | Interaction | |
| Age | 70 ± 4 | 71 ± 4 | 0.33 | ||||
| Nutrition | |||||||
| Energy (kJ/day) | 7201 ± 1892 | 7385 ± 1276 | 7716 ± 991 | 7531 ± 1262 | 0.78 | 0.23 | 0.13 |
| Carbohydrates (g) | 205 ± 38 | 210 ± 43 | 223 ± 37 | 218 ± 39 | 0.98 | 0.15 | 0.34 |
| Fat (g) | 69 ± 33 | 71 ± 22 | 72 ± 11 | 74 ± 15 | 0.20 | 0.19 | 0.34 |
| Protein (g) | 72 ± 25 | 73 ± 15 | 78 ± 12 | 72 ± 15 | 0.67 | 0.35 | 0.06 |
| Physical activity | |||||||
| Chair-stand test (repetitions) | 16 ± 4 | 19 ± 4 | 16 ± 4 | 20 ± 5 | <0.001 | 0.99 | 0.03 |
| Arm-curl test (repetitions) | 19 ± 4 | 24 ± 4 | 19 ± 4 | 24 ± 5 | <0.001 | 0.58 | 0.46 |
| Parameter | ET-Placebo (n = 23–24) | ET-Calanus (n = 27) | Two-Way ANOVA p-Value | ||||
|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Time Effect | Group/Suppl. Effect | Interaction | |
| Fat mass (%) | 38.8 ± 5.2 | 37.4 ± 5.1 *** | 41.4 ± 5.1 | 40.2 ± 5.7 *** | <0.001 | 0.11 | 0.84 |
| Total body weight (kg) | 71.6 ± 12.9 | 70.5 ± 12.7 ** | 71.5 ± 10.1 | 71.0 ± 10.6 | 0.003 | 0.70 | 0.16 |
| Fat mass (kg) | 27.6 ± 8.3 | 26.0 ± 7.9 *** | 29.3 ± 7.7 | 28.2 ± 7.7 *** | <0.001 | 0.31 | 0.70 |
| Lean mass (kg) | 42.0 ± 5.9 | 42.3 ± 5.7 | 40.4 ± 3.4 | 40.9 ± 3.1 * | 0.002 | 0.35 | 0.72 |
| Arm fat (kg) | 3.00 ± 0.99 | 2.89 ± 0.81 | 3.13 ± 0.66 | 3.08 ± 0.79 | 0.15 | 0.34 | 0.97 |
| Leg fat (kg) | 9.23 ± 3.06 | 8.72 ± 2.92 *** | 9.86 ± 2.83 | 9.68 ± 2.71 | <0.001 | 0.23 | 0.05 |
| Trunk fat (kg) | 14.3 ± 4.9 | 13.6 ± 4.6 * | 15.4 ± 5.4 | 14.6 ± 5.2 ** | <0.001 | 0.43 | 0.61 |
| Android fat (kg) | 2.36 ± 0.96 | 2.22 ± 0.89 | 2.49 ± 1.00 | 2.37 ± 1.02 * | <0.001 | 0.50 | 0.43 |
| Gynoid fat (kg) | 4.36 ± 1.23 | 4.14 ± 1.20 ** | 4.77 ± 1.12 | 4.56 ± 1.23 ** | <0.001 | 0.19 | 0.83 |
| Arm fat/total FM (%) | 10.9 ± 1.5 | 11.2 ± 1.5 | 10.9 ± 1.7 | 11.1 ± 1.5 | 0.25 | 0.77 | 0.85 |
| Leg fat/total FM (%) | 33.9 ± 5.6 | 33.6 ± 5.4 | 34.0 ± 5.8 | 35.0 ± 6.2 * | 0.14 | 0.69 | 0.02 |
| Trunk fat/total FM (%) | 51.6 ± 6.1 | 51.6 ± 5.9 | 52.0 ± 5.8 | 50.6 ± 6.4 ** | 0.04 | 0.86 | 0.03 |
| Android fat/total FM (%) | 8.2 ± 1.6 | 8.3 ± 1.6 | 8.3 ± 1.5 | 8.1 ± 1.6 | 0.27 | 0.99 | 0.07 |
| Gynoid fat/total FM (%) | 16.1 ± 2.3 | 16.0 ± 2.0 | 16.4 ± 2.1 | 16.3 ± 2.0 | 0.48 | 0.60 | 0.83 |
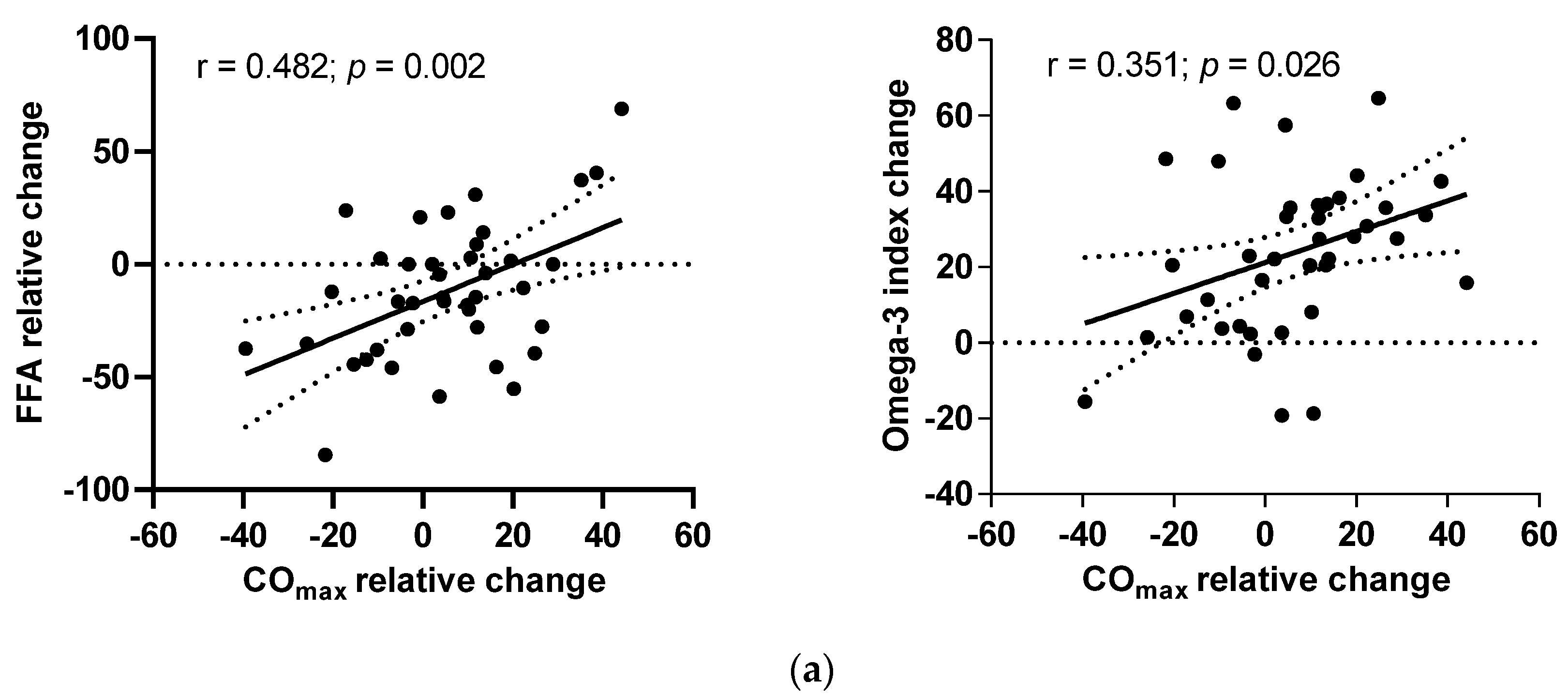
| Plasma FFA (mmol/L) | 0.65 ± 0.24 | 0.51 ± 0.21 * | 0.65 ± 0.24 | 0.61 ± 0.21 | 0.006 | 0.12 | 0.47 |
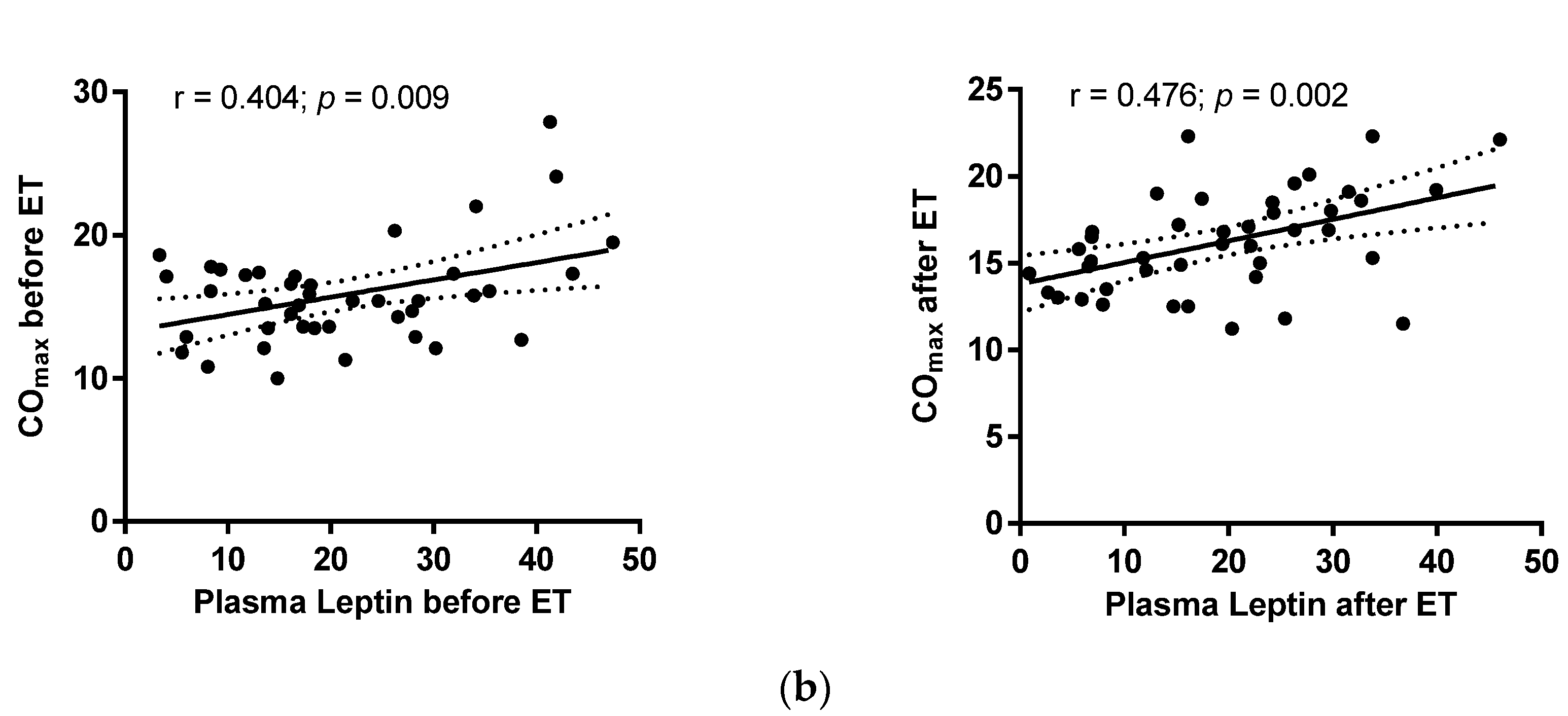
| Plasma Leptin (ng/mL) | 20.3 ± 12.0 | 16.0 ± 10.0 * | 21.1 ± 12.0 | 19.5 ± 11.3 | 0.015 | 0.58 | 0.39 |
| Omega-3 index (%) | 5.22 ± 1.25 | 6.10 ± 1.66 | 4.99 ± 0.98 | 6.39 ± 1.17 | <0.001 | 0.787 | 0.06 |
| Parameter | ET-Placebo (n = 16–24) | ET-Calanus (n = 24–27) | Two-Way ANOVA | ||||
|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Time Effect | Group Effect | Interaction | |
| VO2max (mL/kg/min) | 19.3 ± 3.1 | 22.9 ± 3.1 *** | 19.6 ± 4.2 | 23.0 ± 4.6 *** | <0.001 | 0.92 | 0.71 |
| VEmax (L/min) | 56.8 ± 14.1 | 65.7 ± 14.3 *** | 56.0 ± 8.5 | 70.3 ± 12.1 *** | <0.001 | 0.45 | 0.17 |
| HRrest (bpm) | 70.5 ± 7.1 | 69.0 ± 7.7 | 72.3 ± 11.9 | 71.0 ± 10.4 | 0.37 | 0.52 | 0.86 |
| HRmax (bpm) | 156.1 ± 12.9 | 154.8 ± 11.5 | 152.2 ± 14.3 | 156.3 ± 13.1 ** | 0.14 | 0.72 | 0.011 |
| SVrest (mL per beat) | 75.3 ± 12.4 | 72.6 ± 12.3 | 75.2 ± 16.2 | 77.2 ± 14.2 | 0.87 | 0.61 | 0.16 |
| SVmax (mL per beat) | 104.0 ± 22.4 | 97.8 ± 16.0 | 106.1 ± 21.9 | 114.9 ± 16.5 * | 0.49 | 0.08 | 0.005 |
| COrest (L/min) | 6.03 ± 1.01 | 5.63 ± 1.07 | 6.34 ± 1.60 | 6.17 ± 1.42 | 0.09 | 0.32 | 0.35 |
| COmax (L/min) | 16.0 ± 3.6 | 15.0 ± 2.9 | 15.7 ± 3.5 | 17.0 ± 2.7 * | 0.59 | 0.33 | 0.006 |
| Maximal a-vO2 difference (mL O2/100 mL blood) | 9.0 ± 1.7 | 11.5 ± 2.7 *** | 8.9 ± 2.4 | 9.7 ± 2.4 | <0.001 | 0.17 | 0.049 |
| SVRrest (dys.s/cm2) | 1247 ± 238 | 1210 ± 238 | 1196 ± 216 | 1180 ± 243 | 0.45 | 0.58 | 0.82 |
| SVRmax (dys.s/cm2) | 492 ± 93 | 489 ± 94 | 495 ± 102 | 455 ± 102 | 0.23 | 0.51 | 0.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Štěpán, M.; Daďová, K.; Matouš, M.; Krauzová, E.; Sontáková, L.; Koc, M.; Larsen, T.; Kuda, O.; Štich, V.; Rossmeislová, L.; et al. Exercise Training Combined with Calanus Oil Supplementation Improves the Central Cardiodynamic Function in Older Women. Nutrients 2022, 14, 149. https://doi.org/10.3390/nu14010149
Štěpán M, Daďová K, Matouš M, Krauzová E, Sontáková L, Koc M, Larsen T, Kuda O, Štich V, Rossmeislová L, et al. Exercise Training Combined with Calanus Oil Supplementation Improves the Central Cardiodynamic Function in Older Women. Nutrients. 2022; 14(1):149. https://doi.org/10.3390/nu14010149
Chicago/Turabian StyleŠtěpán, Marek, Klára Daďová, Miloš Matouš, Eva Krauzová, Lenka Sontáková, Michal Koc, Terje Larsen, Ondrej Kuda, Vladimír Štich, Lenka Rossmeislová, and et al. 2022. "Exercise Training Combined with Calanus Oil Supplementation Improves the Central Cardiodynamic Function in Older Women" Nutrients 14, no. 1: 149. https://doi.org/10.3390/nu14010149