The ω-3 Polyunsaturated Fatty Acids and Oxidative Stress in Long-Term Parenteral Nutrition Dependent Adult Patients: Functional Lipidomics Approach

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients and Controls
2.2. Parameters of Oxidative Stress
2.3. Determination of Malondialdehyde Concentration in Plasma and Erythrocytes
2.4. Lipidomics Analysis and Lipid Identification
2.5. Statistical Analyses
3. Results
3.1. Oxidative Stress Markers
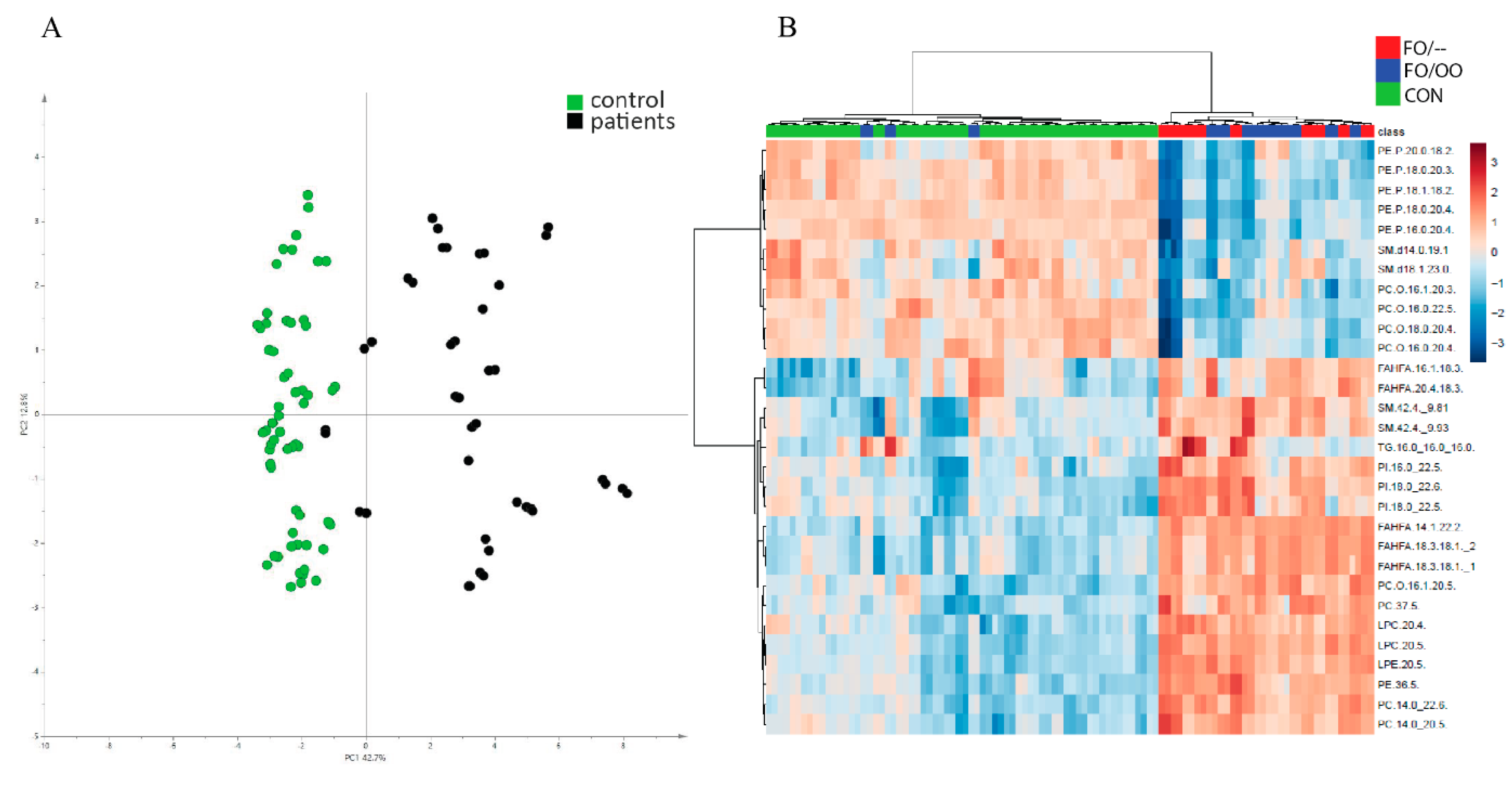
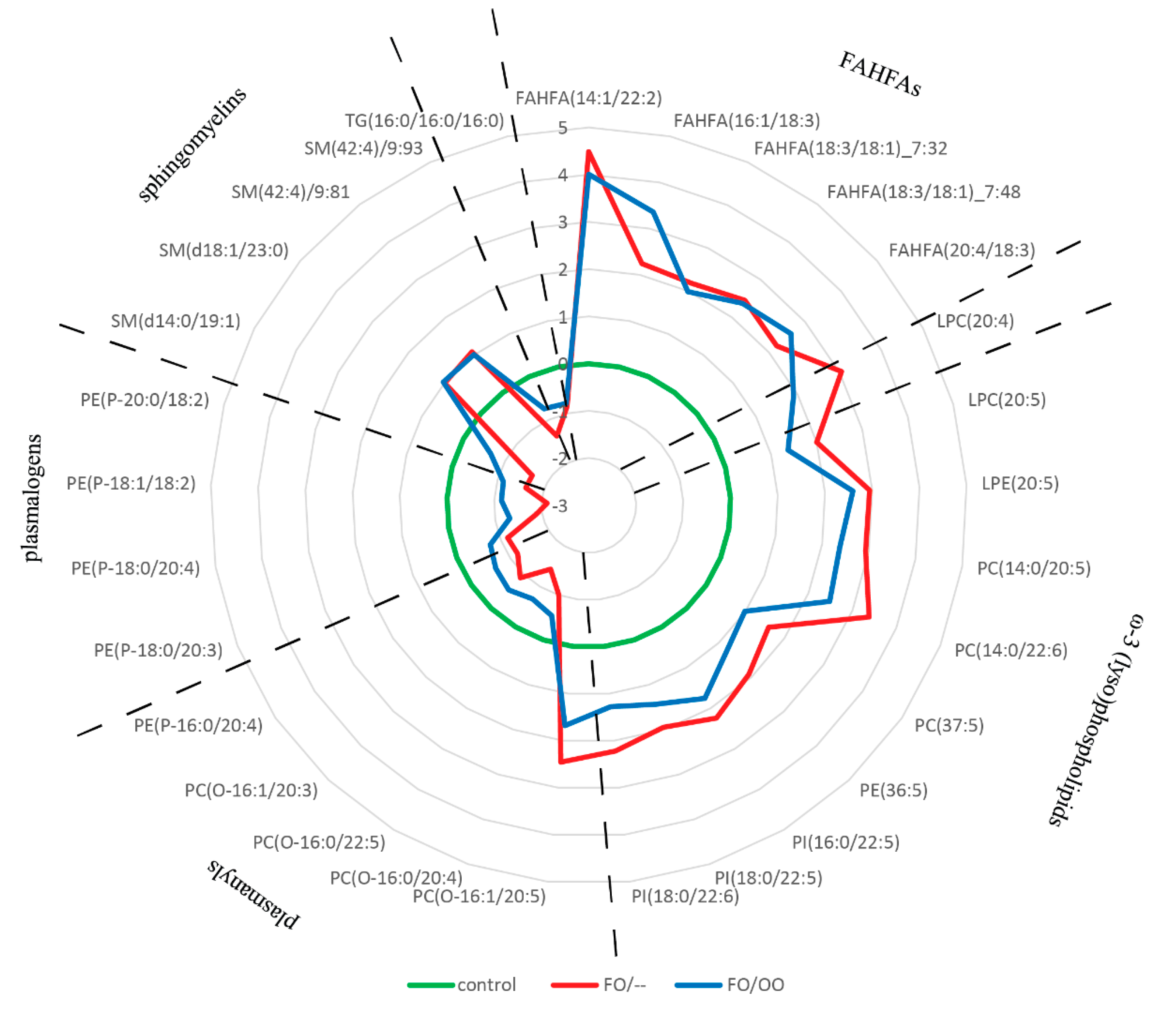
3.2. Lipidomic Analysis: Plasma
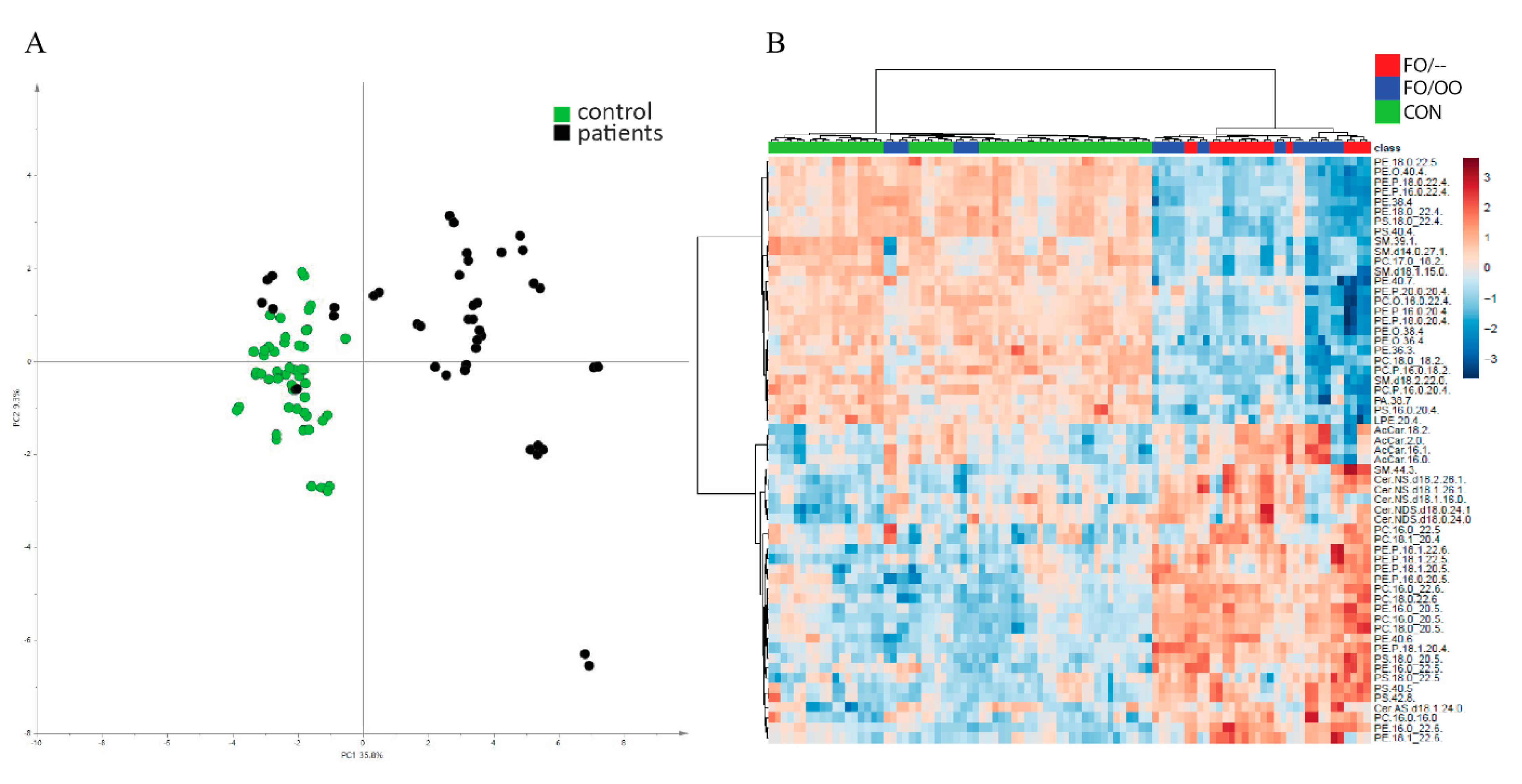
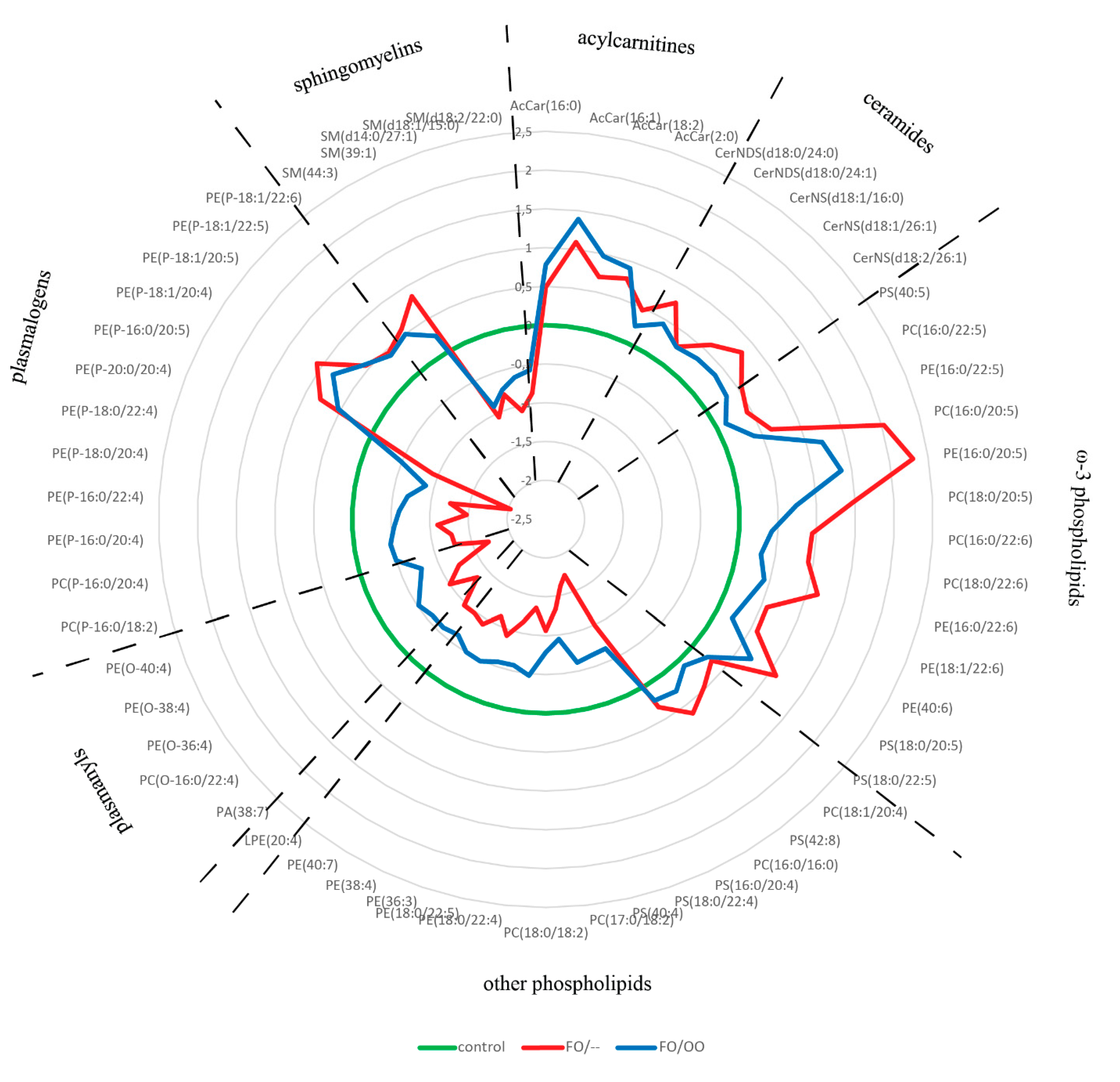
3.3. Lipidomic Analysis: Erythrocytes
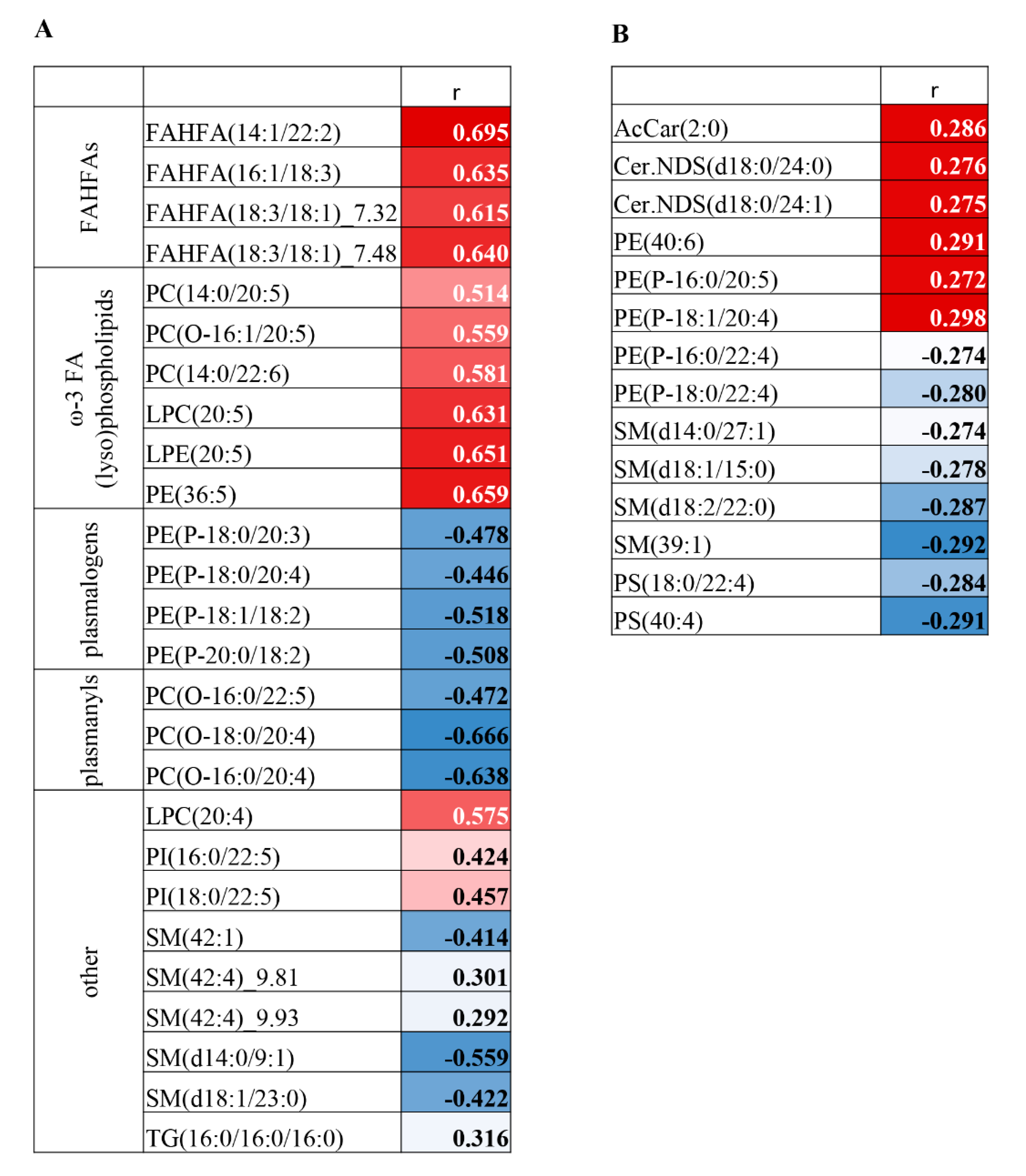
3.4. Correlation Analysis on MDA-Lipidome Level
4. Discussion
4.1. Oxidative Stress in PN-Dependent Patients
4.2. Functional Lipidomics and Biomarkers of Oxidative Stress
4.3. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mizock, B.A. Immunonutrition and critical illness: An update. Nutrition 2010, 26, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Ren, T.; Cong, L.; Wang, Y.; Tang, Y.; Tian, B.; Lin, X.; Zhang, Y.; Tang, X. Lipid emulsions in parenteral nutrition: Current applications and future developments. Expert Opin. Drug Deliv. 2013, 10, 1533–1549. [Google Scholar] [CrossRef] [PubMed]
- Roche, L.D. Oxidative stress: The dark side of soybean-oil-based emulsions used in parenteral nutrition. Oxid. Antioxid. Med. Sci. 2012, 1, 11–14. [Google Scholar] [CrossRef]
- Im, D.S. Omega-3 fatty acids in anti-inflammation (pro-resolution) and GPCRs. Prog. Lipid Res. 2012, 51, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Poudyal, H.; Panchal, S.K.; Diwan, V.; Brown, L. Omega-3 fatty acids and metabolic syndrome: Effects and emerging mechanisms of action. Prog. Lipid Res. 2011, 50, 372–387. [Google Scholar] [CrossRef]
- Klek, S. Omega-3 Fatty Acids in Modern Parenteral Nutrition: A Review of the Current Evidence. J. Clin. Med. 2016, 5, 34. [Google Scholar] [CrossRef] [Green Version]
- Maehre, H.K.; Jensen, I.J.; Elvevoll, E.O.; Eilertsen, K.E. Omega-3 Fatty Acids and Cardiovascular Diseases: Effects, Mechanisms and Dietary Relevance. Int. J. Mol. Sci. 2015, 16, 22636–22661. [Google Scholar] [CrossRef]
- Cai, W.; Calder, P.C.; Cury-Boaventura, M.F.; De Waele, E.; Jakubowski, J.; Zaloga, G. Biological and Clinical Aspects of an Olive Oil-Based Lipid Emulsion-A Review. Nutrients 2018, 10, 776. [Google Scholar] [CrossRef] [Green Version]
- Baena-Gomez, M.A.; Aguilar, M.J.; Mesa, M.D.; Navero, J.L.; Gil-Campos, M. Changes in Antioxidant Defense System Using Different Lipid Emulsions in Parenteral Nutrition in Children after Hematopoietic Stem Cell Transplantation. Nutrients 2015, 7, 7242–7255. [Google Scholar] [CrossRef] [Green Version]
- Linseisen, J.; Hoffmann, J.; Lienhard, S.; Jauch, K.W.; Wolfram, G. Antioxidant status of surgical patients receiving TPN with an omega-3-fatty acid-containing lipid emulsion supplemented with alpha-tocopherol. Clin. Nutr. 2000, 19, 177–184. [Google Scholar] [CrossRef]
- Mostad, I.L.; Bjerve, K.S.; Basu, S.; Sutton, P.; Frayn, K.N.; Grill, V. Addition of n-3 fatty acids to a 4-hour lipid infusion does not affect insulin sensitivity, insulin secretion, or markers of oxidative stress in subjects with type 2 diabetes mellitus. Metabolism 2009, 58, 1753–1761. [Google Scholar] [CrossRef] [PubMed]
- Unal, S.; Demirel, N.; Erol, S.; Isik, D.U.; Kulali, F.; Iyigun, F.; Bas, A.Y. Effects of two different lipid emulsions on morbidities and oxidant stress statuses in preterm infants: An observational study. J. Matern. Fetal Neonatal Med. 2018, 31, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Versleijen, M.W.; Roelofs, H.M.; Rombouts, C.; Hermans, P.W.; Noakes, P.S.; Calder, P.C.; Wanten, G.J. Short-term infusion of a fish oil-based lipid emulsion modulates fatty acid status, but not immune function or (anti)oxidant balance: A randomized cross-over study. Eur. J. Clin. Investig. 2012, 42, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.H.; Lu, S.C.; Wang, T.F.; Jou, H.J.; Wang, T.A. Effects of docosahexaenoic acid supplementation on blood lipids, estrogen metabolism, and in vivo oxidative stress in postmenopausal vegetarian women. Eur. J. Clin. Nutr. 2006, 60, 386–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshpande, G.; Simmer, K.; Deshmukh, M.; Mori, T.A.; Croft, K.D.; Kristensen, J. Fish Oil (SMOFlipid) and olive oil lipid (Clinoleic) in very preterm neonates. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Skouroliakou, M.; Konstantinou, D.; Koutri, K.; Kakavelaki, C.; Stathopoulou, M.; Antoniadi, M.; Xemelidis, N.; Kona, V.; Markantonis, S. A double-blind, randomized clinical trial of the effect of omega-3 fatty acids on the oxidative stress of preterm neonates fed through parenteral nutrition. Eur. J. Clin. Nutr. 2010, 64, 940–947. [Google Scholar] [CrossRef] [Green Version]
- Demirer, S.; Sapmaz, A.; Karaca, A.S.; Kepenekci, I.; Aydintug, S.; Balci, D.; Sonyurek, P.; Kose, K. Effects of postoperative parenteral nutrition with different lipid emulsions in patients undergoing major abdominal surgery. Ann. Surg. Treat. Res. 2016, 91, 309–315. [Google Scholar] [CrossRef] [Green Version]
- Miloudi, K.; Comte, B.; Rouleau, T.; Montoudis, A.; Levy, E.; Lavoie, J.C. The mode of administration of total parenteral nutrition and nature of lipid content influence the generation of peroxides and aldehydes. Clin. Nutr. 2012, 31, 526–534. [Google Scholar] [CrossRef]
- Arisue, A.; Shimojima, N.; Tomiya, M.; Shimizu, T.; Harada, D.; Nakayama, M.; Tomita, H.; Shinoda, M.; Tanabe, M.; Maruyama, I.; et al. Effect of an omega-3 lipid emulsion in reducing oxidative stress in a rat model of intestinal ischemia-reperfusion injury. Pediatr. Surg. Int. 2012, 28, 913–918. [Google Scholar] [CrossRef] [Green Version]
- Lavoie, J.C.; Mohamed, I.; Nuyt, A.M.; Elremaly, W.; Rouleau, T. Impact of SMOFLipid on Pulmonary Alveolar Development in Newborn Guinea Pigs. JPEN J. Parenter. Enteral. Nutr. 2018, 42, 1314–1321. [Google Scholar] [CrossRef]
- Zhang, T.; Wang, N.; Yan, W.; Lu, L.; Tao, Y.; Li, F.; Wang, Y.; Cai, W. Effect of a fish oil-based lipid emulsion on intestinal failure-associated liver disease in children. Eur. J. Clin. Nutr. 2018, 72, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Pironi, L.; Guidetti, M.; Verrastro, O.; Iacona, C.; Agostini, F.; Pazzeschi, C.; Sasdelli, A.S.; Melchiorre, M.; Ferreri, C. Functional lipidomics in patients on home parenteral nutrition: Effect of lipid emulsions. World J. Gastroenterol. 2017, 23, 4604–4614. [Google Scholar] [CrossRef]
- Klek, S.; Chambrier, C.; Singer, P.; Rubin, M.; Bowling, T.; Staun, M.; Joly, F.; Rasmussen, H.; Strauss, B.J.; Wanten, G.; et al. Four-week parenteral nutrition using a third generation lipid emulsion (SMOFlipid)—A double-blind, randomised, multicentre study in adults. Clin. Nutr. 2013, 32, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Rolim, A.E.; Henrique-Araujo, R.; Ferraz, E.G.; de Araujo Alves Dultra, F.K.; Fernandez, L.G. Lipidomics in the study of lipid metabolism: Current perspectives in the omic sciences. Gene 2015, 554, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Pironi, L.; Arends, J.; Baxter, J.; Bozzetti, F.; Pelaez, R.B.; Cuerda, C.; Forbes, A.; Gabe, S.; Gillanders, L.; Holst, M.; et al. ESPEN endorsed recommendations. Definition and classification of intestinal failure in adults. Clin. Nutr. 2015, 34, 171–180. [Google Scholar] [CrossRef]
- Iuliano, L.; Piccheri, C.; Coppola, I.; Pratico, D.; Micheletta, F.; Violi, F. Fluorescence quenching of dipyridamole associated to peroxyl radical scavenging: A versatile probe to measure the chain breaking antioxidant activity of biomolecules. Biochim. Biophys. Acta 2000, 1474, 177–182. [Google Scholar] [CrossRef]
- Chen, Z.; Wang, S.; Yu, B.; Li, A. A comparison study between early enteral nutrition and parenteral nutrition in severe burn patients. Burns 2007, 33, 708–712. [Google Scholar] [CrossRef]
- Hagen, T.M. Oxidative stress, redox imbalance, and the aging process. Antioxid. Redox Signal. 2003, 5, 503–506. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Zalewska, A.; Ladny, J.R. Salivary Antioxidant Barrier, Redox Status, and Oxidative Damage to Proteins and Lipids in Healthy Children, Adults, and the Elderly. Oxid. Med. Cell Longev. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Pajares, M.; Cuadrado, A.; Engedal, N.; Jirsova, Z.; Cahova, M. The Role of Free Radicals in Autophagy Regulation: Implications for Ageing. Oxid. Med. Cell Longev. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Bruna, E.; Petit, E.; Beljeanleymarie, M.; Huynh, S.; Nouvelot, A. Specific Susceptibility of Docosahexaenoic Acid and Eicosapentaenoic Acid to Peroxidation in Aqueous-Solution. Lipids 1989, 24, 970–975. [Google Scholar] [CrossRef]
- Fuhrman, B.; Volkova, N.; Aviram, M. Postprandial. serum triacylglycerols and oxidative stress in mice after consumption of fish oil, soy oil or olive oil: Possible role for paraoxonase-1 triacylglycerol lipase-like activity. Nutrition 2006, 22, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Lauriti, G.; Zani, A.; Aufieri, R.; Cananzi, M.; Chiesa, P.L.; Eaton, S.; Pierro, A. Incidence, prevention, and treatment of parenteral nutrition-associated cholestasis and intestinal failure-associated liver disease in infants and children: A systematic review. JPEN J. Parenter. Enteral. Nutr. 2014, 38, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Nanhuck, R.M.; Doublet, A.; Yaqoob, P. Effects of lipid emulsions on lipid body formation and eicosanoid production by human peripheral blood mononuclear and polymorphonuclear cells. Clin. Nutr. 2009, 28, 556–564. [Google Scholar] [CrossRef]
- Watkins, S.M.; Carter, L.C.; German, J.B. Docosahexaenoic acid accumulates in cardiolipin and enhances HT-29 cell oxidant production. J. Lipid Res. 1998, 39, 1583–1588. [Google Scholar]
- Lessig, J.; Fuchs, B. Plasmalogens in biological systems: Their role in oxidative processes in biological membranes, their contribution to pathological processes and aging and plasmalogen analysis. Curr. Med. Chem. 2009, 16, 2021–2041. [Google Scholar] [CrossRef]
- Braverman, N.E.; Moser, A.B. Functions of plasmalogen lipids in health and disease. Biochim. Biophys. Acta 2012, 1822, 1442–1452. [Google Scholar] [CrossRef] [Green Version]
- Sindelar, P.J.; Guan, Z.; Dallner, G.; Ernster, L. The protective role of plasmalogens in iron-induced lipid peroxidation. Free Radic. Biol. Med. 1999, 26, 318–324. [Google Scholar] [CrossRef]
- Hu, C.; Zhou, J.; Yang, S.; Li, H.; Wang, C.; Fang, X.; Fan, Y.; Zhang, J.; Han, X.; Wen, C. Oxidative stress leads to reduction of plasmalogen serving as a novel biomarker for systemic lupus erythematosus. Free Radic. Biol. Med. 2016, 101, 475–481. [Google Scholar] [CrossRef]
- Maeba, R.; Nishimukai, M.; Sakasegawa, S.; Sugimori, D.; Hara, H. Plasma/Serum Plasmalogens: Methods of Analysis and Clinical Significance. Adv. Clin. Chem. 2015, 70, 31–94. [Google Scholar] [CrossRef]
- Yore, M.M.; Syed, I.; Moraes-Vieira, P.M.; Zhang, T.; Herman, M.A.; Homan, E.A.; Patel, R.T.; Lee, J.; Chen, S.; Peroni, O.D.; et al. Discovery of a class of endogenous mammalian lipids with anti-diabetic and anti-inflammatory effects. Cell 2014, 159, 318–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, A.T.; Kolar, M.J.; Chu, Q.; Syed, I.; Kahn, B.B.; Saghatelian, A.; Siegel, D. Stereochemistry of Endogenous Palmitic Acid Ester of 9-Hydroxystearic Acid and Relevance of Absolute Configuration to Regulation. J. Am. Chem. Soc. 2017, 139, 4943–4947. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | FO/– | FO/OO | |
|---|---|---|---|
| sex (F/M) | 20/10 | 7/2 | 10/3 |
| age (years) | 64 (40;80) | 60 (32;73) | 66 (42;81) |
| BMI | 25.7 (19.3;30.2) | 25 (18;28) | 21 (16;30) |
| time on PN (month) | N/A | 40 (2;113) | 56 (7;124) |
| CRP (mg/l) | 0.9 (0.1;6.5) | 1.6 * (0.3;7.3) | 1.1 * (0.9;13.6) |
| diagnosis | |||
| SBS I | N/A | 7 | 3 |
| SBS II + III | N/A | 2 | 4 |
| other | N/A | 0 | 6 |
| parenteral nutrition | |||
| i.v. energy (kcal/day) | N/A | 940 (568;1575) | 1144 (545;1705) |
| lipids (g/day) | N/A | 20 (5.7;50) | 32.2 (5.7;56.3) |
| soybean oil (g/day) | N/A | 8.0 (2.3;20) | 9.7 (1.7;16.9) |
| olive oil (g/day) | N/A | 0.0 | 8.1 ‡ (1.4;15.2) |
| MCFA (g/day) | N/A | 10.0 (2.9;25) | 9.7 (1.7;16.9) |
| fish oil (g/day) | N/A | 2.0 (0.6;5.0) | 4.6 (0.9;8.4) |
| amino acids (g/day) | N/A | 50.0 (28.6;71.5) | 53.6 (28.6;108.6) |
| glucose (g/day) | N/A | 138 (71;250) | 134 (36;200) |
| lipid metabolism | |||
| TAG (mmol/L) | 1.5 (0.8;3.6) | 1.6 (1.1;2.6) | 1.2 (0.5;2.4) |
| total cholesterol (mmol/L) | 5.3 (3.6;7.6) | 3.3 (2.6;4.3) | 3.8 (2.0;4.5) |
| HDL cholesterol (mmol/L) | 2.2 (0.9;6.1) | 1.1 (0.5;1.4) | 1.2 (1.0;2.1) |
| LDL cholesterol (mmol/L) | 2.0 (1.0;4.3) | 1.6 * (0.8;2.3) | 1.6 * (1.0;2.3) |
| liver function tests | |||
| bilirubin (µmol/L) | 9.9 (4.8;27.3) | 13.0 (6.7;33.1) | 9.5 (5.1;88.1) |
| AST (µkat/L) | 0.4 (0.3;1.8) | 0.5 (0.4;1.4) | 0.4 (0.3;2.5) |
| ALT (µkat/L) | 0.6 (0.4;1.1) | 0.8 (0.4;4.1) | 0.4 (0.3;1.0) |
| ALP (µkat/L) | 1.3 (0.7;2.1) | 2.2 (1.4;3.1) | 1.9 (1.1;2.7) |
| GGT (µkat/L) | 0.4 (0.2;1.8) | 0.7 (0.2;2.9) | 0.6 (0.2;2.2) |
| albumin (g/L) | 42 (35;47) | 43 (39;48) | 44 (36;53) |
| other | |||
| blood count | 4.4 (3.9;5.2) | 3.9 (3.4;4.8) | 4.3 (2.8;5.1) |
| uric acid | 253 (180;287) | 268 (179;573) | 236 (116;353) |
| total protein content | 70 (58;81) | 73 (68;83) | 71 (67;81) |
| Control | FO/– | FO/OO | ||
|---|---|---|---|---|
| oxidative stress markers | ||||
| erythrocytes | MDA (nmol·g Hb−1) | 7.4 (5.1;10.9) | 14.3 *** (7.0;31.9) | 13.8 *** (5.0;35.9) |
| protein carbonyls (nmol·mg Hb−1) | 0.4 (0.0;1.1) | 0.7 (0.3;1.2) | 0.4 (0.3;1.1) | |
| non-enzymatic oxidants | ||||
| antioxidant capacity | 16.0 (10.0;21.6) | 15.6 (9.2;18.4) | 15.6 (11.6;21.6) | |
| GSH | 1430 (847;2398) | 1187 (789;2059) | 1736 (947;2215) | |
| GSSG | 57.5 (29.1;97.8) | 64.3 (33.3;116.5) | 74.1 (38.1;109.6) | |
| redox status | ||||
| GSH/GSSG | 25.3 † (11.0;44.1) | 17.7 * (15.1;22.3) | 24.8 † (15.7;41.4) | |
| oxidative stress markers | ||||
| plasma | MDA (µM) | 1.4 (1.0;1.9) | 2.3 *** (1.6;3.4) | 2.1 *** (1.2;3.4) |
| protein carbonyls (nmol mg Hb−1) | 1.8 † (0.0;4.2) | 2.9 * (1.0;6.3) | 1.3 † (0.5;5.3) | |
| non-enzymatic oxidants | ||||
| antioxidant capacity | 59.6 (41.6;79) | 55.2 (41.2;114) | 47.2 (37.6;67.2) | |
| antioxidant enzymes | ||||
| SOD (U/ml) | 1.8 (1.1;2.2) | 1.5 (1.1;2.0) | 2.0 (1.3;2.3) | |
| GSH-Px (µM NADPH/min/ml) | 330 (280;360) | 375 (330;410) | 370 (310;440) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosek, V.; Heczkova, M.; Novak, F.; Meisnerova, E.; Novákova, O.; Zelenka, J.; Bechynska, K.; Vrzacova, N.; Suttnar, J.; Hlavackova, A.; et al. The ω-3 Polyunsaturated Fatty Acids and Oxidative Stress in Long-Term Parenteral Nutrition Dependent Adult Patients: Functional Lipidomics Approach. Nutrients 2020, 12, 2351. https://doi.org/10.3390/nu12082351
Kosek V, Heczkova M, Novak F, Meisnerova E, Novákova O, Zelenka J, Bechynska K, Vrzacova N, Suttnar J, Hlavackova A, et al. The ω-3 Polyunsaturated Fatty Acids and Oxidative Stress in Long-Term Parenteral Nutrition Dependent Adult Patients: Functional Lipidomics Approach. Nutrients. 2020; 12(8):2351. https://doi.org/10.3390/nu12082351
Chicago/Turabian StyleKosek, Vit, Marie Heczkova, Frantisek Novak, Eva Meisnerova, Olga Novákova, Jaroslav Zelenka, Kamila Bechynska, Nikola Vrzacova, Jiri Suttnar, Alzbeta Hlavackova, and et al. 2020. "The ω-3 Polyunsaturated Fatty Acids and Oxidative Stress in Long-Term Parenteral Nutrition Dependent Adult Patients: Functional Lipidomics Approach" Nutrients 12, no. 8: 2351. https://doi.org/10.3390/nu12082351