
Influence of COVID-19-Related Restrictions on the Prevalence of Overweight and Obese Czech Children
Abstract
:1. Introduction
2. Materials and Methods
2.1. Background
2.2. Data Collection
2.3. Measurement
2.4. Statistical Analyses
- is the BMI of child i that is measured in year t at age a
- is an overall intercept (unknown parameter to be estimated from data)
- is the random effect of the i-th child ()
- is the random error of child i that is measured in year t at age a ()
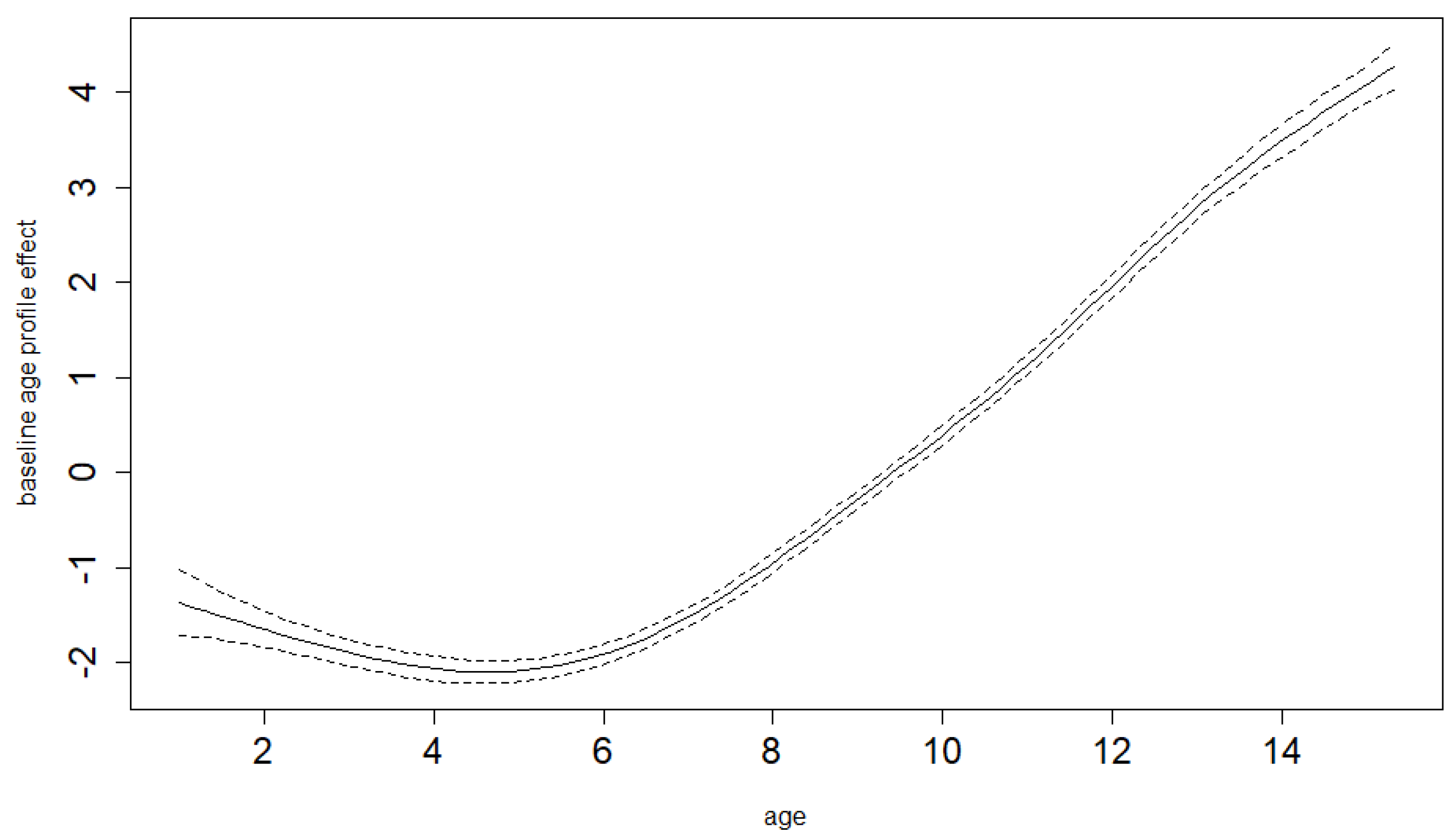
- is the baseline (pre-COVID-19 year) mean BMI age profile (unknown smooth function to be estimated from the data)
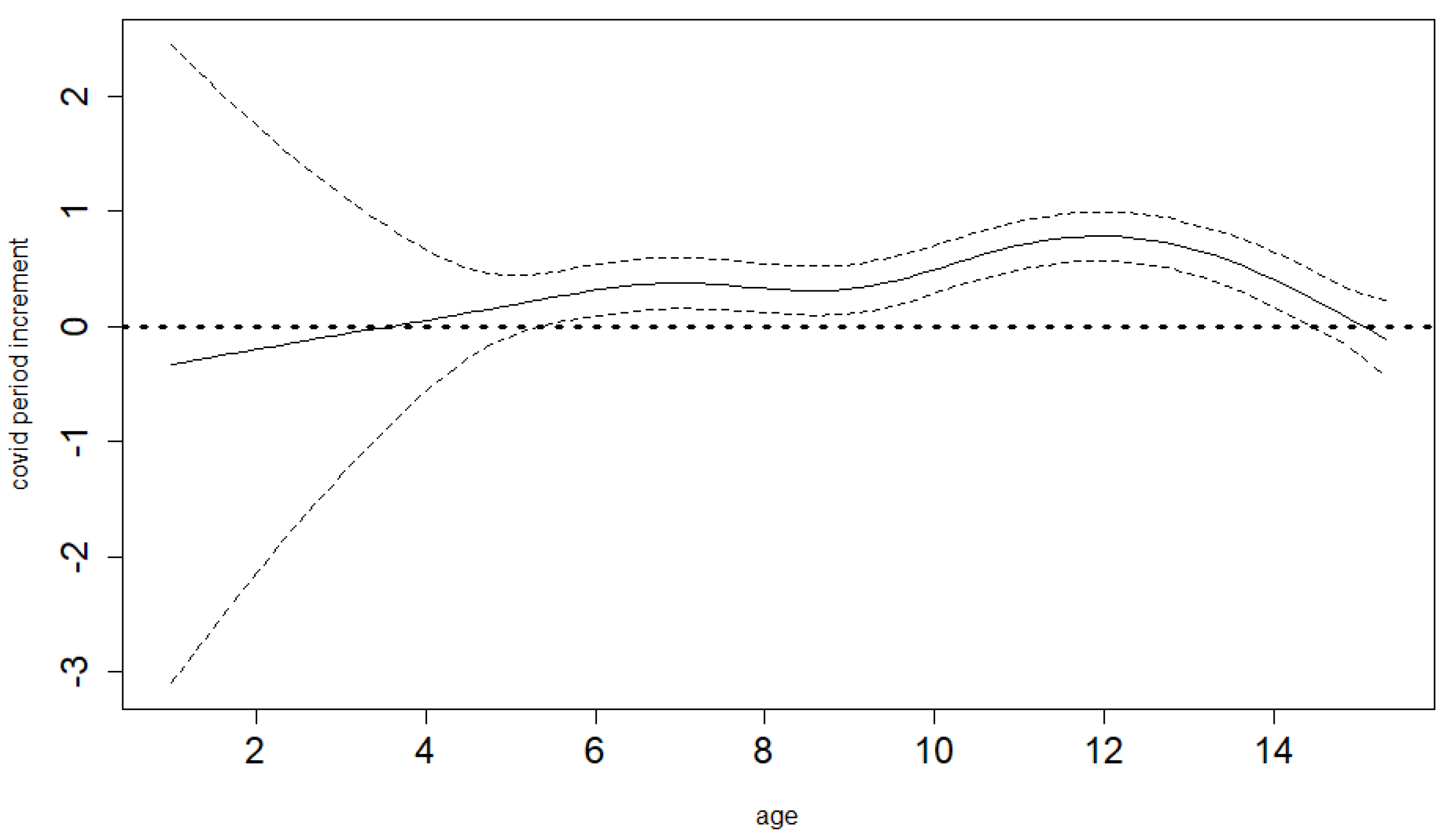
- is the age-differential increment in BMI in COVID-19-year (unknown smooth function to be estimated from the data)
- is an indicator function (assuming the value of 1 if its argument is true and the value of 0 otherwise)
2.5. Ethical Considerations
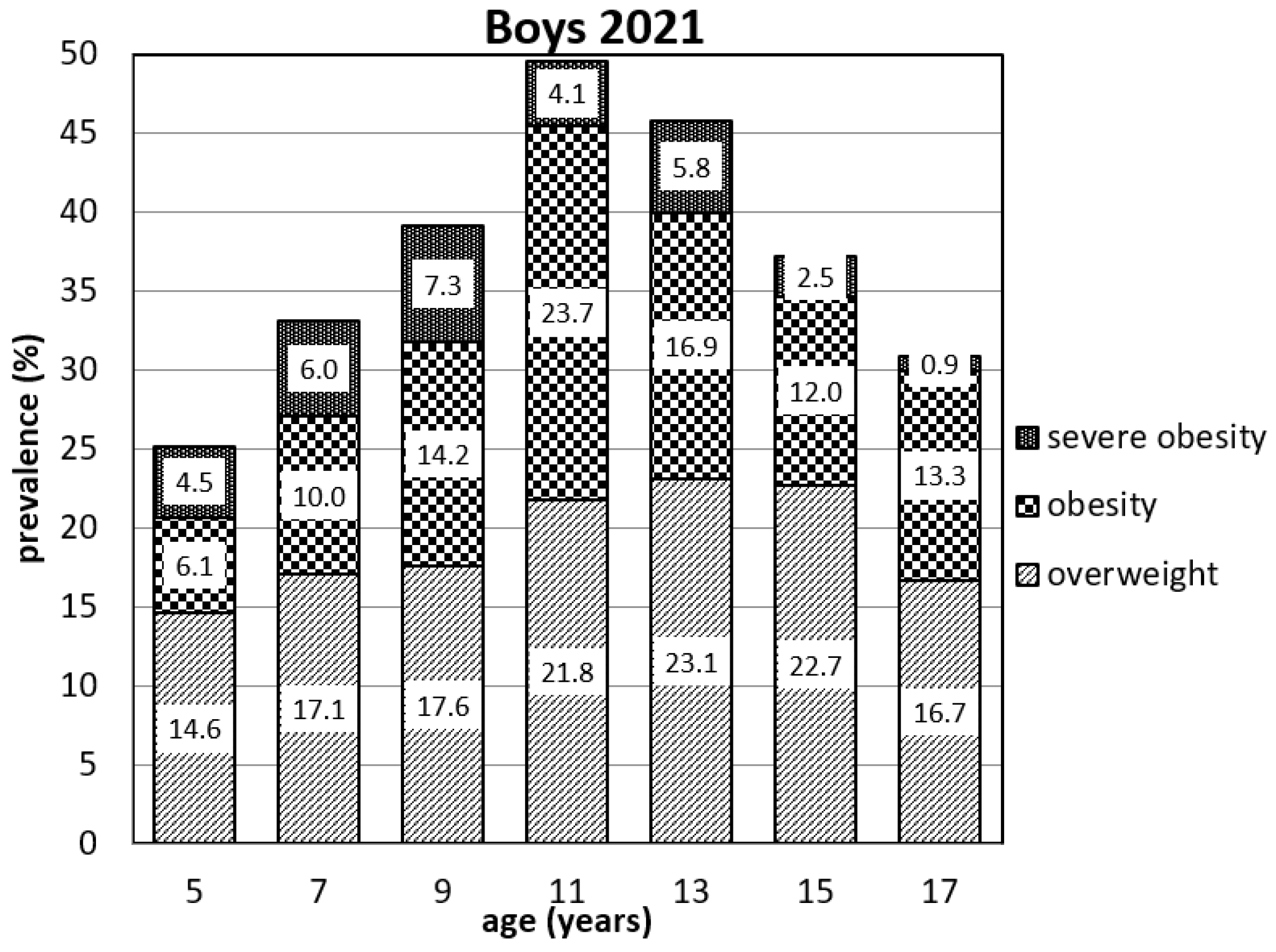
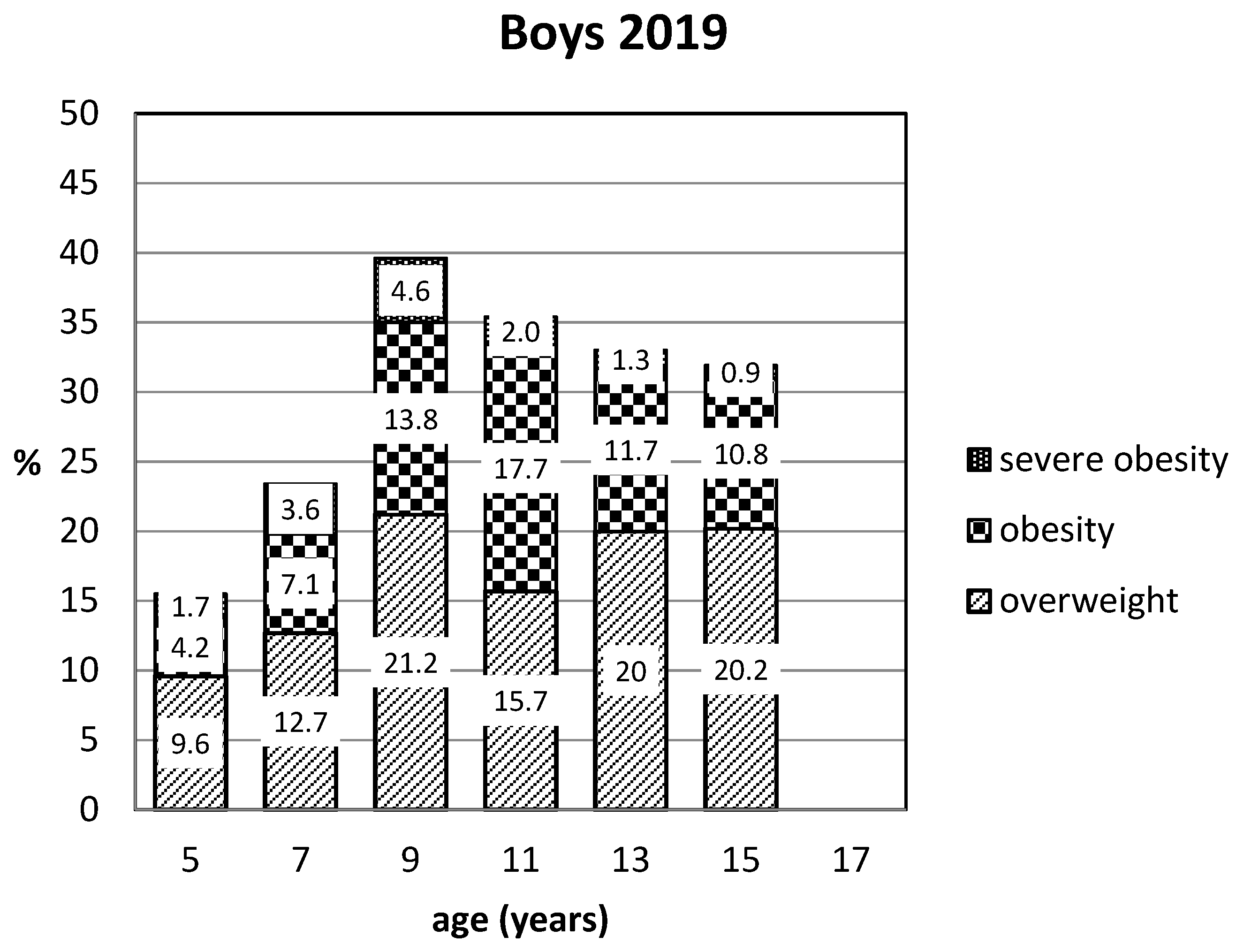
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Final Age (Years) | 2021 Visit | 2019 Visit | 2017 Visit | 2015 Visit | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | n | Mean | SEM | n | Mean | SEM | n | Mean | SEM | n | Mean | SEM | |
| 5 | boys | 246 | 15.96 | 4.61 | 244 | 15.94 | 3.78 | 98 | 16.28 | 3.16 | 0 | ||
| girls | 245 | 15.70 | 4.61 | 242 | 15.68 | 3.78 | 107 | 16.36 | 3.15 | 0 | |||
| 7 | boys | 251 | 16.74 | 3.94 | 250 | 15.53 | 2.28 | 240 | 15.93 | 2.59 | 89 | 16.75 | 2.73 |
| girls | 243 | 16.49 | 4.61 | 240 | 15.45 | 1.36 | 232 | 15.59 | 2.09 | 67 | 16.19 | 2.60 | |
| 9 | boys | 261 | 18.02 | 3.46 | 261 | 16.15 | 2.11 | 253 | 15.47 | 2.45 | 224 | 15.85 | 1.47 |
| girls | 254 | 17.65 | 3.56 | 251 | 16.13 | 2.20 | 248 | 15.68 | 2.58 | 215 | 15.72 | 2.59 | |
| 11 | boys | 266 | 20.27 | 3.86 | 265 | 17.88 | 2.69 | 260 | 16.46 | 2.41 | 232 | 15.64 | 1.32 |
| girls | 266 | 19.53 | 3.89 | 261 | 17.45 | 2.68 | 254 | 16.12 | 2.39 | 235 | 15.57 | 1.38 | |
| 13 | boys | 260 | 21.44 | 4.61 | 254 | 19.08 | 2.64 | 251 | 17.44 | 2.36 | 232 | 16.05 | 1.35 |
| girls | 269 | 21.23 | 4.10 | 266 | 18.93 | 3.23 | 265 | 17.37 | 2.76 | 231 | 16.12 | 2.33 | |
| 15 | boys | 242 | 22.14 | 4.98 | 237 | 20.21 | 4.32 | 233 | 18.60 | 3.53 | 222 | 17.11 | 3.20 |
| girls | 254 | 21.07 | 5.00 | 252 | 19.76 | 4.27 | 245 | 17.91 | 3.51 | 232 | 16.51 | 2.58 | |
| 17 | boys | 233 | 23.18 | 4.90 | 231 | 21.89 | 4.14 | 227 | 20.39 | 3.38 | 214 | 18.99 | 2.58 |
| girls | 227 | 22.21 | 4.97 | 222 | 21.27 | 4.15 | 218 | 20.09 | 3.36 | 208 | 18.21 | 2.30 | |


| 2021 (n = 494) | 2015 (n = 451) | COSI (2015–17) (n = 1002) | ||||
|---|---|---|---|---|---|---|
| Obese | Overweight | Obese | Overweight | Obese | Overweight | |
| boys | 15.9 | 17.1 | 11.9 | 11.1 | 10.9 | 12 |
| girls | 9.5 | 19.3 | 8.9 | 11.1 | 5.5 | 14.6 |
References
- World Health Organization Origin of SARS-CoV-2. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/332197/WHO-2019-nCoV-FAQ-Virus_origin-2020.1-eng.pdf?sequence=1&isAllowed=y (accessed on 20 May 2022).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in Lifestyle Behaviours during the COVID-19 Confinement in Spanish Children: A Longitudinal Analysis from the MUGI Project. Pediat. Obes. 2021, 16, e12731. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.-P.; Bentham, J. The Epidemiological Burden of Obesity in Childhood: A Worldwide Epidemic Requiring Urgent Action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef]
- Campagnaro, R.; de Oliveira Collet, G.; de Andrade, M.P.; Salles, J.P.D.S.L.; Calvo Fracasso, M.D.L.; Scheffel, D.L.S.; Freitas, K.M.S.; Santin, G.C. COVID-19 Pandemic and Pediatric Dentistry: Fear, Eating Habits and Parent’s Oral Health Perceptions. Child. Youth Serv. Rev. 2020, 118, 105469. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Sioen, I.; Braet, C.; Eiben, G.; Hebestreit, A.; Huybrechts, I.; Vanaelst, B.; Vyncke, K.; De Henauw, S. Stress, Emotional Eating Behaviour and Dietary Patterns in Children. Appetite 2012, 59, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 Virus Outbreak on Movement and Play Behaviours of Canadian Children and Youth: A National Survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef]
- Baranowski, T.; O’Connor, T.; Johnston, C.; Hughes, S.; Moreno, J.; Chen, T.-A.; Meltzer, L.; Baranowski, J. School Year Versus Summer Differences in Child Weight Gain: A Narrative Review. Child. Obes. 2014, 10, 18–24. [Google Scholar] [CrossRef]
- Moreno, J.P.; Johnston, C.A.; Woehler, D. Changes in Weight Over the School Year and Summer Vacation: Results of a 5-Year Longitudinal Study. J. School Health 2013, 83, 473–477. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Brazendale, K.; Beets, M.W.; Weaver, R.G.; Pate, R.R.; Turner-McGrievy, G.M.; Kaczynski, A.T.; Chandler, J.L.; Bohnert, A.; von Hippel, P.T. Understanding Differences between Summer vs. School Obesogenic Behaviors of Children: The Structured Days Hypothesis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- von Hippel, P.T.; Workman, J. From Kindergarten Through Second Grade, U.S. Children’s Obesity Prevalence Grows Only During Summer Vacations: Obesity Grows Only During Summer. Obesity 2016, 24, 2296–2300. [Google Scholar] [CrossRef] [PubMed]
- Bac, A.; Woźniacka, R.; Matusik, S.; Golec, J.; Golec, E. Prevalence of Overweight and Obesity in Children Aged 6–13 Years—Alarming Increase in Obesity in Cracow, Poland. Eur. J. Pediatr. 2012, 171, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of Obesity and Trends in Body Mass Index Among US Children and Adolescents, 1999–2010. JAMA 2012, 307, 483. [Google Scholar] [CrossRef]
- de Onis, M. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.J.; Tibshirani, R.J. Generalized Additive Models, 1st ed.; Chapman and Hall/CRC: London, UK, 1990; ISBN 978-0-412-34390-2. [Google Scholar]
- Wood, S.N.; Li, Z.; Shaddick, G.; Augustin, N.H. Generalized Additive Models for Gigadata: Modeling the U.K. Black Smoke Network Daily Data. JASA 2017, 112, 1199–1210. [Google Scholar] [CrossRef]
- Wood, S.N. Just Another Gibbs Additive Modeller: Interfacing JAGS and Mgcv. arXiv 2016, arXiv:1602.02539. [Google Scholar] [CrossRef]
- Laird, N.M.; Ware, J.H. Random-Effects Models for Longitudinal Data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef]
- Ghanemi, A.; Yoshioka, M.; St-Amand, J. Will an Obesity Pandemic Replace the Coronavirus Disease-2019 (COVID-19) Pandemic? Med. Hypotheses 2020, 144, 110042. [Google Scholar] [CrossRef]
- Guan, H.; Okely, A.D.; Aguilar-Farias, N.; del Pozo Cruz, B.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Jáuregui, A.; Katzmarzyk, P.T.; Kontsevaya, A.; et al. Promoting Healthy Movement Behaviours among Children during the COVID-19 Pandemic. Lancet Child Adolesc. Health 2020, 4, 416–418. [Google Scholar] [CrossRef]
- Nagata, J.M.; Abdel Magid, H.S.; Pettee Gabriel, K. Screen Time for Children and Adolescents During the Coronavirus Disease 2019 Pandemic. Obesity 2020, 28, 1582–1583. [Google Scholar] [CrossRef] [PubMed]
- Storz, M.A. The COVID-19 Pandemic: An Unprecedented Tragedy in the Battle against Childhood Obesity. Clin. Exp. Pediatr. 2020, 63, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Kimm, S.Y.S.; Obarzanek, E. Childhood Obesity: A New Pandemic of the New Millennium. Pediatrics 2002, 110, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- Browne, N.T.; Snethen, J.A.; Greenberg, C.S.; Frenn, M.; Kilanowski, J.F.; Gance-Cleveland, B.; Burke, P.J.; Lewandowski, L. When Pandemics Collide: The Impact of COVID-19 on Childhood Obesity. J. Pediatr. Nurs. 2021, 56, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.J.; Aris, I.M.; Hivert, M.-F.; Rocchio, C.; Cocoros, N.M.; Klompas, M.; Taveras, E.M. Association of Changes in Obesity Prevalence With the COVID-19 Pandemic in Youth in Massachusetts. JAMA Pediatr. 2022, 176, 198. [Google Scholar] [CrossRef]
- Jenssen, B.P.; Kelly, M.K.; Powell, M.; Bouchelle, Z.; Mayne, S.L.; Fiks, A.G. COVID-19 and Changes in Child Obesity. Pediatrics 2021, 147, e2021050123. [Google Scholar] [CrossRef]
- World Health Organisation. WHO European Childhood Obesity Surveillance Initiative (COSI), Report on the Fourth Round of Data Collection, 2015–2017. 2021. Available online: https://apps.who.int/iris/handle/10665/341189 (accessed on 20 May 2022).
- Stavridou, A.; Kapsali, E.; Panagouli, E.; Thirios, A.; Polychronis, K.; Bacopoulou, F.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Obesity in Children and Adolescents during COVID-19 Pandemic. Children 2021, 8, 135. [Google Scholar] [CrossRef]
- Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef]
- Tester, J.M.; Rosas, L.G.; Leung, C.W. Food Insecurity and Pediatric Obesity: A Double Whammy in the Era of COVID-19. Curr. Obes. Rep. 2020, 9, 442–450. [Google Scholar] [CrossRef]
- Pujia, R.; Ferro, Y.; Maurotti, S.; Khoory, J.; Gazzaruso, C.; Pujia, A.; Montalcini, T.; Mazza, E. The Effects of COVID-19 on the Eating Habits of Children and Adolescents in Italy: A Pilot Survey Study. Nutrients 2021, 13, 2641. [Google Scholar] [CrossRef] [PubMed]
- Zenic, N.; Taiar, R.; Gilic, B.; Blazevic, M.; Maric, D.; Pojskic, H.; Sekulic, D. Levels and Changes of Physical Activity in Adolescents during the COVID-19 Pandemic: Contextualizing Urban vs. Rural Living Environment. Appl. Sci. 2020, 10, 3997. [Google Scholar] [CrossRef]
- Kovacs, V.A.; Starc, G.; Brandes, M.; Kaj, M.; Blagus, R.; Leskošek, B.; Suesse, T.; Dinya, E.; Guinhouya, B.C.; Zito, V.; et al. Physical Activity, Screen Time and the COVID-19 School Closures in Europe—An Observational Study in 10 Countries. Eur. J. Sport Sci. 2022, 22, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.C.E.; Anedda, B.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Nigg, C.; Niessner, C.; Oriwol, D.; Worth, A.; Woll, A. Physical Activity and Screen Time of Children and Adolescents before and during the COVID-19 Lockdown in Germany: A Natural Experiment. Sci. Rep. 2020, 10, 21780. [Google Scholar] [CrossRef] [PubMed]
- McArthur, B.A.; Racine, N.; Browne, D.; McDonald, S.; Tough, S.; Madigan, S. Recreational Screen Time before and during COVID-19 in School-aged Children. Acta Paediatr. 2021, 110, 2805–2807. [Google Scholar] [CrossRef]
- Dunger, D.B.; Lynn Ahmed, M.; Ong, K.K. Effects of Obesity on Growth and Puberty. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 375–390. [Google Scholar] [CrossRef]
- Ahmed, M.L.; Ong, K.K.; Dunger, D.B. Childhood Obesity and the Timing of Puberty. Trends Endocrinol. Metab. 2009, 20, 237–242. [Google Scholar] [CrossRef]
- Pérusse, L.; Chagnon, Y.C.; Dionne, F.T.; Bouchard, C. The Human Obesity Gene Map: The 1996 Update. Obes. Res. 1997, 5, 49–61. [Google Scholar] [CrossRef]
- Shalitin, S.; Phillip, M. Role of Obesity and Leptin in the Pubertal Process and Pubertal Growth—A Review. Int. J. Obes. 2003, 27, 869–874. [Google Scholar] [CrossRef]
- Novak, J.M.; Bruzek, J.; Zamrazilova, H.; Vankova, M.; Hill, M.; Sedlak, P. The Relationship between Adolescent Obesity and Pelvis Dimensions in Adulthood: A Retrospective Longitudinal Study. PeerJ 2020, 8, e8951. [Google Scholar] [CrossRef]
- Milner, J.J.; Beck, M.A. The Impact of Obesity on the Immune Response to Infection. Proc. Nutr. Soc. 2012, 71, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with Obesity and COVID-19: A Global Perspective on the Epidemiology and Biological Relationships. Obesity Reviews 2020, 21, e13128. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.; Burch, J.; Llewellyn, A.; Griffiths, C.; Yang, H.; Owen, C.; Duffy, S.; Woolacott, N. The Use of Measures of Obesity in Childhood for Predicting Obesity and the Development of Obesity-Related Diseases in Adulthood: A Systematic Review and Meta-Analysis. Health Technol. Assess. 2015, 19, 1–336. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; Van Mechelen, W.; Chinapaw, M.J.M. Tracking of Childhood Overweight into Adulthood: A Systematic Review of the Literature: Tracking of Childhood Overweight into Adulthood. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]






| Final Age (y) | 2021 Visit | 2021–2019 Diff | 2019 Visit | 2019–2017 Diff | 2017 Visit | 2017–2015 Diff | 2015 Visit | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | n | Mean | SEM | D-C | p-Value | n | Mean | SEM | D-C | p-Value | n | Mean | SEM | D-C | p-Value | n | Mean | SEM | |
| 5 | boys | 246 | 0.42 | 0.09 | 1.94 | 0.054 | 244 | 0.21 | 0.07 | 1.72 | 0.086 | 98 | 0.03 | 0.10 | 0 | ||||
| girls | 245 | 0.16 | 0.08 | 0.44 | 0.656 | 242 | 0.13 | 0.07 | 1.30 | 0.193 | 107 | 0.33 | 0.12 | 0 | |||||
| 7 | boys | 251 | 0.56 | 0.10 | 3.67 | 0.0003 | 250 | 0.13 | 0.08 | 2.25 | 0.024 | 240 | 0.19 | 0.09 | 2.17 | 0.031 | 89 | 0.34 | 0.12 |
| girls | 243 | 0.40 | 0.08 | 2.61 | 0.009 | 240 | 0.02 | 0.07 | 1.89 | 0.060 | 232 | 0.06 | 0.07 | 0.89 | 0.373 | 67 | 0.24 | 0.13 | |
| 9 | boys | 261 | 0.70 | 0.09 | 6.96 | <0.00001 | 261 | 0.23 | 0.09 | 0.50 | 0.615 | 253 | 0.10 | 0.07 | 1.31 | 0.189 | 224 | 0.16 | 0.07 |
| girls | 254 | 0.4 | 0.09 | 3.73 | 0.0002 | 251 | 0.19 | 0.08 | 0.05 | 0.954 | 248 | 0.15 | 0.08 | 1.33 | 0.182 | 215 | 0.15 | 0.08 | |
| 11 | boys | 266 | 1.01 | 0.09 | 5.76 | <0.00001 | 265 | 0.68 | 0.08 | 2.97 | 0.003 | 260 | 0.43 | 0.08 | 0.21 | 0.831 | 232 | 0.23 | 0.07 |
| girls | 266 | 0.55 | 0.08 | 3.55 | 0.0004 | 261 | 0.36 | 0.08 | 2.07 | 0.038 | 254 | 0.22 | 0.07 | 2.03 | 0.041 | 235 | 0.05 | 0.07 | |
| 13 | boys | 260 | 0.72 | 0.10 | 3.11 | 0.002 | 254 | 0.56 | 0.09 | 1.07 | 0.280 | 251 | 0.45 | 0.09 | 3.3 | 0.001 | 232 | 0.16 | 0.10 |
| girls | 269 | 0.56 | 0.07 | 3.02 | 0.002 | 266 | 0.40 | 0.07 | 0.85 | 0.390 | 265 | 0.34 | 0.07 | 2.72 | 0.006 | 231 | 0.21 | 0.08 | |
| 15 | boys | 242 | 0.53 | 0.08 | 1.31 | 0.190 | 237 | 0.43 | 0.09 | 1.10 | 0.270 | 233 | 0.45 | 0.08 | 2.09 | 0.036 | 222 | 0.33 | 0.09 |
| girls | 254 | 0.09 | 0.07 | 0.52 | 0.590 | 252 | 0.11 | 0.07 | 0.68 | 0.490 | 245 | 0.05 | 0.07 | 0.05 | 0.950 | 232 | 0.01 | 0.07 | |
| 17 | boys | 233 | 0.43 | 0.08 | 0.98 | 0.320 | 231 | 0.49 | 0.08 | 0.64 | 0.510 | 227 | 0.52 | 0.09 | 2.35 | 0.010 | 214 | 0.64 | 0.09 |
| girls | 227 | 0.18 | 0.07 | 0.94 | 0.340 | 222 | 0.18 | 0.07 | 1.53 | 0.120 | 218 | 0.22 | 0.08 | 2.32 | 0.020 | 208 | 0.13 | 0.09 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vážná, A.; Vignerová, J.; Brabec, M.; Novák, J.; Procházka, B.; Gabera, A.; Sedlak, P. Influence of COVID-19-Related Restrictions on the Prevalence of Overweight and Obese Czech Children. Int. J. Environ. Res. Public Health 2022, 19, 11902. https://doi.org/10.3390/ijerph191911902
Vážná A, Vignerová J, Brabec M, Novák J, Procházka B, Gabera A, Sedlak P. Influence of COVID-19-Related Restrictions on the Prevalence of Overweight and Obese Czech Children. International Journal of Environmental Research and Public Health. 2022; 19(19):11902. https://doi.org/10.3390/ijerph191911902
Chicago/Turabian StyleVážná, Anna, Jana Vignerová, Marek Brabec, Jan Novák, Bohuslav Procházka, Antonín Gabera, and Petr Sedlak. 2022. "Influence of COVID-19-Related Restrictions on the Prevalence of Overweight and Obese Czech Children" International Journal of Environmental Research and Public Health 19, no. 19: 11902. https://doi.org/10.3390/ijerph191911902